

A new workflow of the on-line 1.5-T MR-guided adaptive radiation therapy
- PMID: 37354344
- PMCID: PMC10613593
- DOI: 10.1007/s11604-023-01457-4
A new workflow of the on-line 1.5-T MR-guided adaptive radiation therapy
Abstract
Purpose: The aim of this study was to develop a new workflow for 1.5-T magnetic resonance (MR)-guided on-line adaptive radiation therapy (MRgART) and assess its feasibility in achieving dose constraints.
Materials and methods: We retrospectively evaluated the clinical data of patients who underwent on-line adaptive radiation therapy using a 1.5-T MR linear accelerator (MR-Linac). The workflow in MRgART was established by reviewing the disease site, number of fractions, and re-planning procedures. Five cases of prostate cancer were selected to evaluate the feasibility of the new workflow with respect to achieving dose constraints.
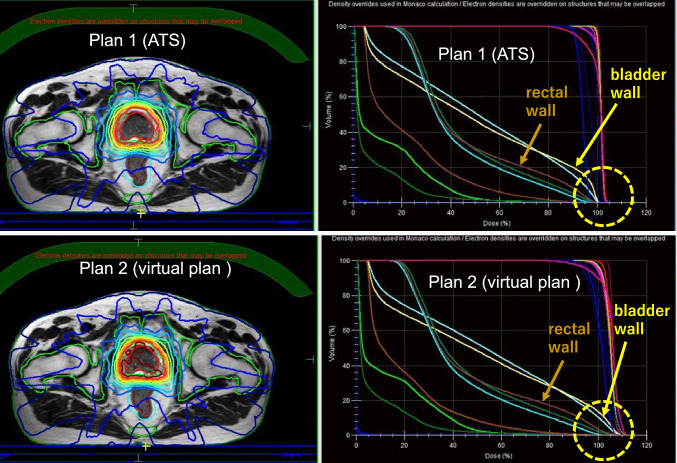
Results: Between December 2021 and September 2022, 50 consecutive patients underwent MRgART using a 1.5-T MR-Linac. Of these, 20 had prostate cancer, 10 had hepatocellular carcinoma, 6 had pancreatic cancer, 5 had lymph node oligo-metastasis, 3 had renal cancer, 3 had bone metastasis, 2 had liver metastasis from colon cancer, and 1 had a mediastinal tumor. Among a total of 247 fractions, 235 (95%) were adapt-to-shape (ATS)-based re-planning. The median ATS re-planning time in all 50 cases was 17 min. In the feasibility study, all dose constraint sets were met in all 5 patients by ATS re-planning. Conversely, a total of 14 dose constraints in 5 patients could not be achieved by virtual plan without using adaptive re-planning. These dose constraints included the minimum dose received by the highest irradiated volume of 1 cc in the planning target volume and the maximum dose of the rectal/bladder wall.
Conclusion: A new workflow of 1.5-T MRgART was established and found to be feasible. Our evaluation of the dose constraint achievement demonstrated the effectiveness of the workflow.
Keywords: Adapt to shape; Adaptive radiation therapy; MR-Linac; MRgART; Workflow.
© 2023. The Author(s).
Conflict of interest statement
The three authors (MT, KA, and YF) belong to an endowed chair sponsored by Elekta Corporation. The other authors have no conflict of interest.
Figures


References
-
- Raaymakers BW, Jürgenliemk-Schulz IM, Bol GH, Glitzner M, Kotte ANTJ, van Asselen B, et al. First patients treated with a 1.5 T MRI-Linac: clinical proof of concept of a high-precision, high-field MRI guided radiotherapy treatment. Phys Med Biol. 2017;62:L41–50. doi: 10.1088/1361-6560/aa9517. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
