

Once-Weekly Insulin Icodec vs Once-Daily Insulin Degludec in Adults With Insulin-Naive Type 2 Diabetes: The ONWARDS 3 Randomized Clinical Trial
- PMID: 37354562
- PMCID: PMC10354685
- DOI: 10.1001/jama.2023.11313
Once-Weekly Insulin Icodec vs Once-Daily Insulin Degludec in Adults With Insulin-Naive Type 2 Diabetes: The ONWARDS 3 Randomized Clinical Trial
Abstract
Importance: Once-weekly insulin icodec could provide a simpler dosing alternative to daily basal insulin in people with type 2 diabetes.
Objective: To evaluate the efficacy and safety of once-weekly icodec vs once-daily insulin degludec in people with insulin-naive type 2 diabetes.
Design, setting, and participants: Randomized, double-masked, noninferiority, treat-to-target, phase 3a trial conducted from March 2021 to June 2022 at 92 sites in 11 countries in adults with type 2 diabetes treated with any noninsulin glucose-lowering agents with hemoglobin A1c (HbA1c) of 7%-11% (53-97 mmol/mol).
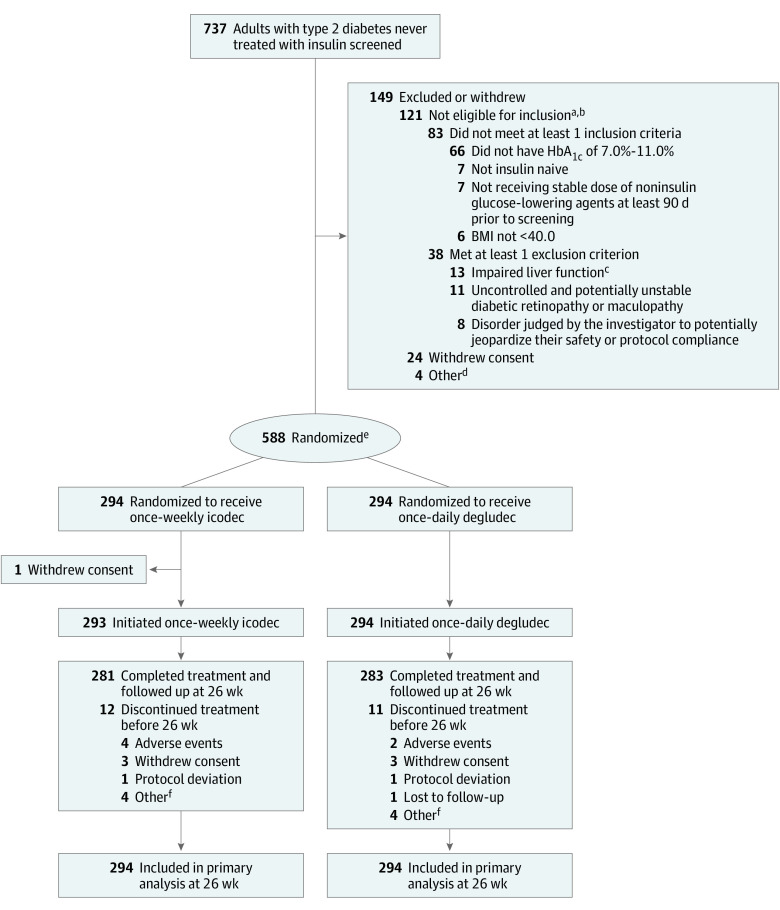
Interventions: Participants were randomly assigned in a 1:1 ratio to receive either once-weekly icodec and once-daily placebo (icodec group; n = 294) or once-daily degludec and once-weekly placebo (degludec group; n = 294).
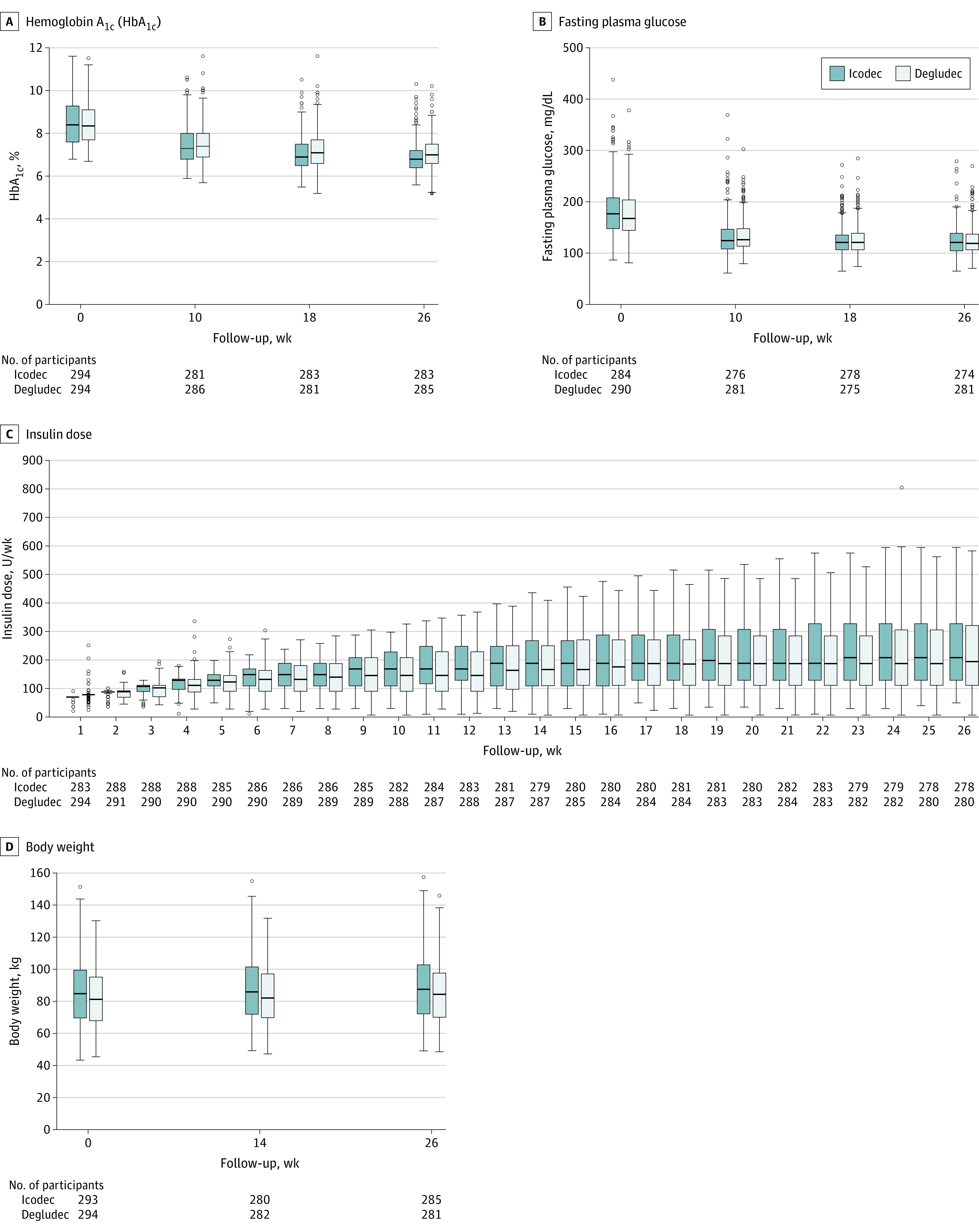
Main outcomes and measures: The primary end point was change in HbA1c from baseline to week 26 (noninferiority margin, 0.3% percentage points). Secondary end points included change in fasting plasma glucose from baseline to week 26, mean weekly insulin dose during the last 2 weeks of treatment, body weight change from baseline to week 26, and number of level 2 (clinically significant; glucose level <54 mg/dL) and level 3 (severe; requiring external assistance for recovery) hypoglycemic episodes.
Results: Among 588 randomized participants (mean [SD] age, 58 [10] years; 219 [37%] women), 564 (96%) completed the trial. Mean HbA1c level decreased from 8.6% (observed) to 7.0% (estimated) at 26 weeks in the icodec group and from 8.5% (observed) to 7.2% (estimated) in the degludec group (estimated treatment difference [ETD], -0.2 [95% CI, -0.3 to -0.1] percentage points), confirming noninferiority (P < .001) and superiority (P = .002). There were no significant differences between the icodec and degludec groups for fasting plasma glucose change from baseline to week 26 (ETD, 0 [95% CI, -6 to 5] mg/dL; P = .90), mean weekly insulin dose during the last 2 weeks of treatment, or body weight change from baseline to week 26 (2.8 kg vs 2.3 kg; ETD, 0.46 [95% CI, -0.19 to 1.10] kg; P = .17). Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than the degludec group from week 0 to 31 (0.31 vs 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs 0.12 events per patient-year exposure; P = .01).
Conclusions and relevance: Among people with insulin-naive type 2 diabetes, once-weekly icodec demonstrated superior HbA1c reduction to once-daily degludec after 26 weeks of treatment, with no difference in weight change and a higher rate of combined level 2 or 3 hypoglycemic events in the context of less than 1 event per patient-year exposure in both groups.
Trial registration: ClinicalTrials.gov Identifier: NCT04795531.
Conflict of interest statement
Figures
Comment in
-
In T2DM uncontrolled with noninsulin glucose-lowering agents, weekly icodec reduced HbA1c vs. daily degludec at 26 wk.Ann Intern Med. 2023 Oct;176(10):JC112. doi: 10.7326/J23-0078. Epub 2023 Oct 3. Ann Intern Med. 2023. PMID: 37782923
References
-
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-2786. doi: 10.2337/dci22-0034 - DOI - PMC - PubMed
-
- Bajaj HS, Bergenstal RM, Christoffersen A, et al. Switching to once-weekly insulin icodec versus once-daily insulin glargine U100 in type 2 diabetes inadequately controlled on daily basal insulin: a phase 2 randomized controlled trial. Diabetes Care. 2021;44(7):1586-1594. doi: 10.2337/dc20-2877 - DOI - PMC - PubMed
