

Predicting in-hospital mortality after transcatheter aortic valve replacement using administrative data and machine learning
- PMID: 37355688
- PMCID: PMC10290690
- DOI: 10.1038/s41598-023-37358-9
Predicting in-hospital mortality after transcatheter aortic valve replacement using administrative data and machine learning
Abstract
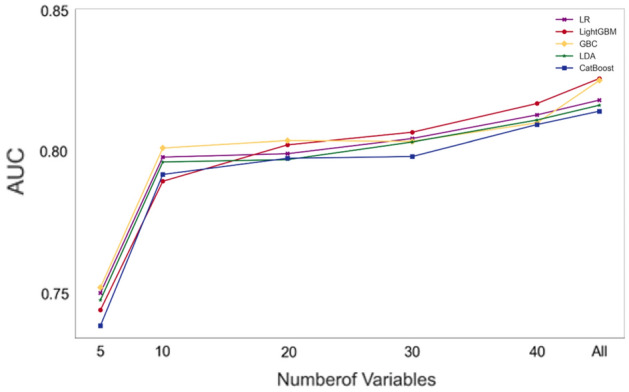
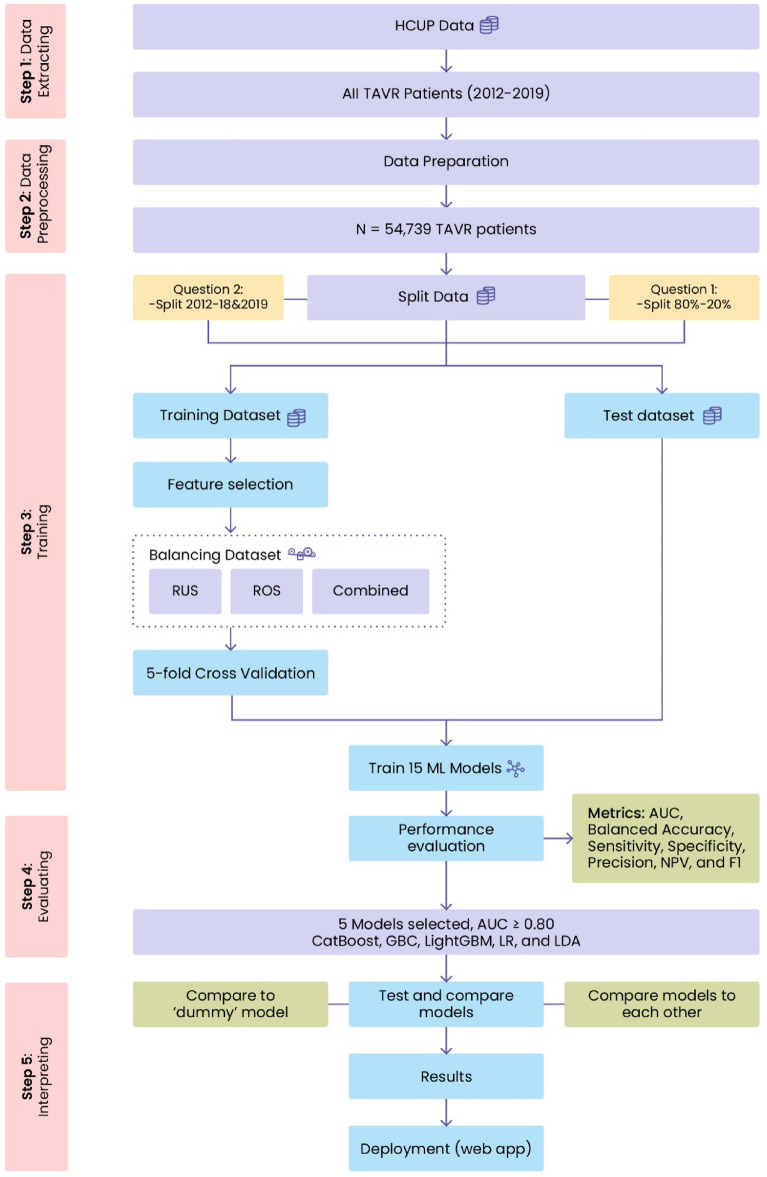
Transcatheter aortic valve replacement (TAVR) is the gold standard treatment for patients with symptomatic aortic stenosis. The utility of existing risk prediction tools for in-hospital mortality post-TAVR is limited due to two major factors: (a) the predictive accuracy of these tools is insufficient when only preoperative variables are incorporated, and (b) their efficacy is also compromised when solely postoperative variables are employed, subsequently constraining their application in preoperative decision support. This study examined whether statistical/machine learning models trained with solely preoperative information encoded in the administrative National Inpatient Sample database could accurately predict in-hospital outcomes (death/survival) post-TAVR. Fifteen popular binary classification methods were used to model in-hospital survival/death. These methods were evaluated using multiple classification metrics, including the area under the receiver operating characteristic curve (AUC). By analyzing 54,739 TAVRs, the top five classification models had an AUC ≥ 0.80 for two sampling scenarios: random, consistent with previous studies, and time-based, which assessed whether the models could be deployed without frequent retraining. Given the minimal practical differences in the predictive accuracies of the top five models, the L2 regularized logistic regression model is recommended as the best overall model since it is computationally efficient and easy to interpret.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Machine Learning Prediction Models for In-Hospital Mortality After Transcatheter Aortic Valve Replacement.JACC Cardiovasc Interv. 2019 Jul 22;12(14):1328-1338. doi: 10.1016/j.jcin.2019.06.013. JACC Cardiovasc Interv. 2019. PMID: 31320027 Free PMC article.
-
Utilization and outcomes of transcatheter aortic valve replacement in the United States shortly after device approval.Catheter Cardiovasc Interv. 2017 Nov 1;90(5):830-838. doi: 10.1002/ccd.27018. Epub 2017 Mar 22. Catheter Cardiovasc Interv. 2017. PMID: 28326675
-
Validation of STS/ACC TVT-TAVR Score in Veterans Undergoing Transcatheter Aortic Valve Replacement.J Invasive Cardiol. 2018 Dec;30(12):447-451. Epub 2018 Sep 15. J Invasive Cardiol. 2018. PMID: 30218556
-
Predicting and measuring mortality risk after transcatheter aortic valve replacement.Expert Rev Cardiovasc Ther. 2021 Mar;19(3):247-260. doi: 10.1080/14779072.2021.1888715. Epub 2021 Mar 2. Expert Rev Cardiovasc Ther. 2021. PMID: 33560150 Review.
-
Transcatheter aortic valve replacement for structural degeneration of previously implanted transcatheter valves (TAVR-in-TAVR): a systematic review.Eur J Cardiothorac Surg. 2022 May 2;61(5):967-976. doi: 10.1093/ejcts/ezab443. Eur J Cardiothorac Surg. 2022. PMID: 34662376
Cited by
-
The role of artificial intelligence in aortic valve stenosis: a bibliometric analysis.Front Cardiovasc Med. 2025 Feb 12;12:1521464. doi: 10.3389/fcvm.2025.1521464. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40013126 Free PMC article.
-
The Current Landscape of Artificial Intelligence in Imaging for Transcatheter Aortic Valve Replacement.Curr Radiol Rep. 2024;12(11-12):113-120. doi: 10.1007/s40134-024-00431-w. Epub 2024 Oct 10. Curr Radiol Rep. 2024. PMID: 39483792 Free PMC article.
-
Predicting mortality after transcatheter aortic valve replacement using preprocedural CT.Sci Rep. 2024 May 31;14(1):12526. doi: 10.1038/s41598-024-63022-x. Sci Rep. 2024. PMID: 38822074 Free PMC article.
-
Futility in TAVI: A scoping review of definitions, predictive criteria, and medical predictive models.PLoS One. 2025 Jan 9;20(1):e0313399. doi: 10.1371/journal.pone.0313399. eCollection 2025. PLoS One. 2025. PMID: 39787130 Free PMC article.
-
Artificial Intelligence in Risk Stratification and Outcome Prediction for Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis.J Pers Med. 2025 Jul 11;15(7):302. doi: 10.3390/jpm15070302. J Pers Med. 2025. PMID: 40710419 Free PMC article. Review.
References
-
- National Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP) (Agency for Healthcare Research and Quality, 2022). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
