

The FGF21 analog pegozafermin in severe hypertriglyceridemia: a randomized phase 2 trial
- PMID: 37355760
- PMCID: PMC10353930
- DOI: 10.1038/s41591-023-02427-z
The FGF21 analog pegozafermin in severe hypertriglyceridemia: a randomized phase 2 trial
Erratum in
-
Author Correction: The FGF21 analog pegozafermin in severe hypertriglyceridemia: a randomized phase 2 trial.Nat Med. 2024 Jun;30(6):1788-1789. doi: 10.1038/s41591-024-02890-2. Nat Med. 2024. PMID: 38438737 Free PMC article. No abstract available.
Abstract
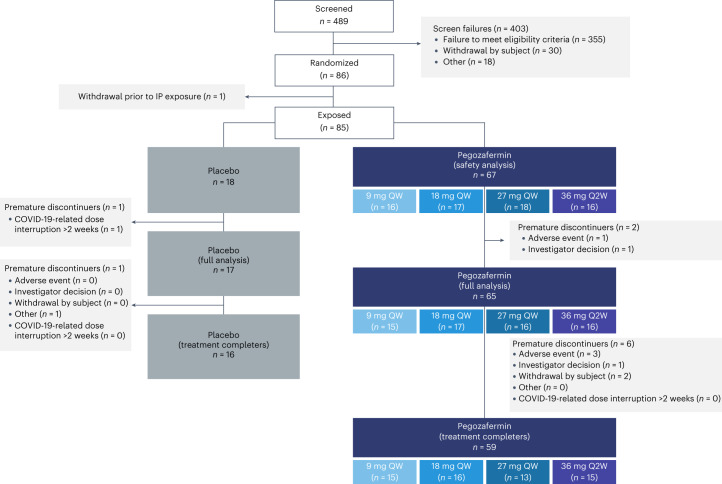
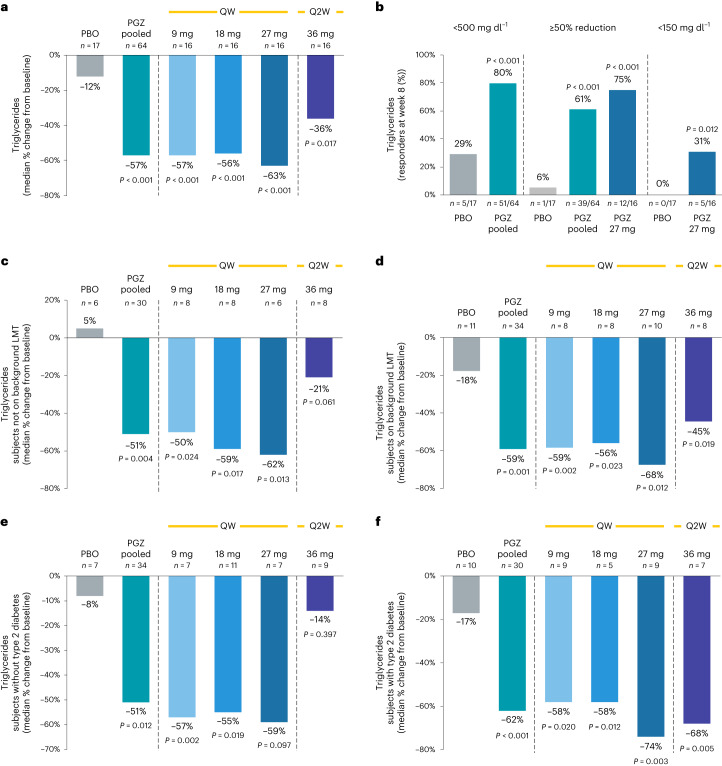
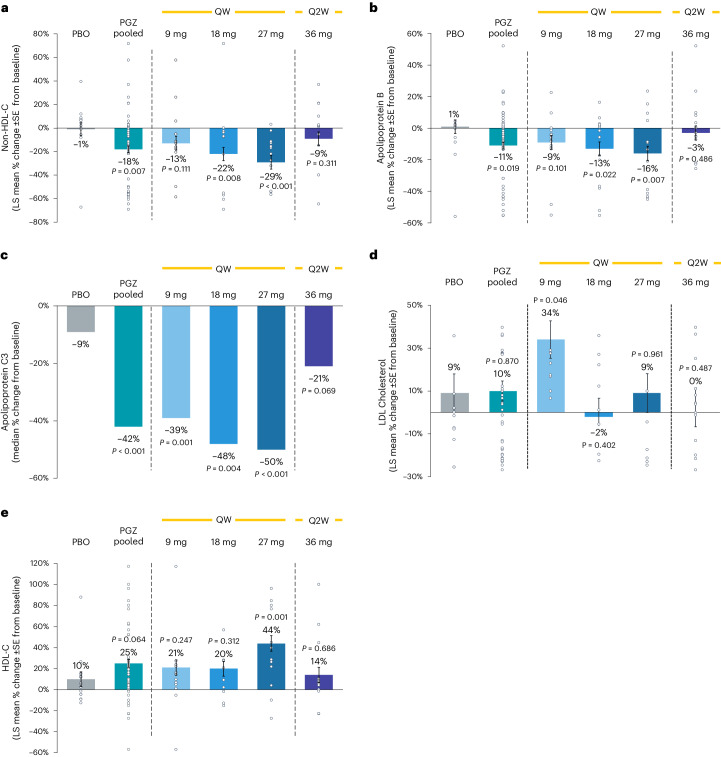
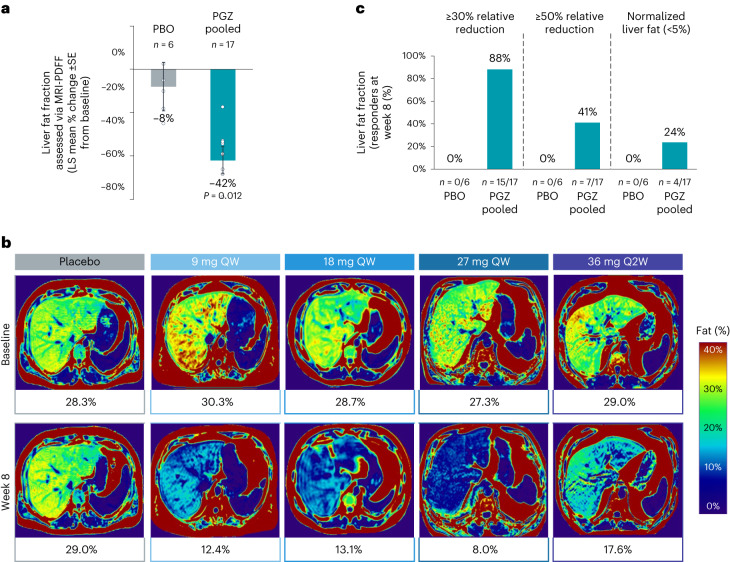
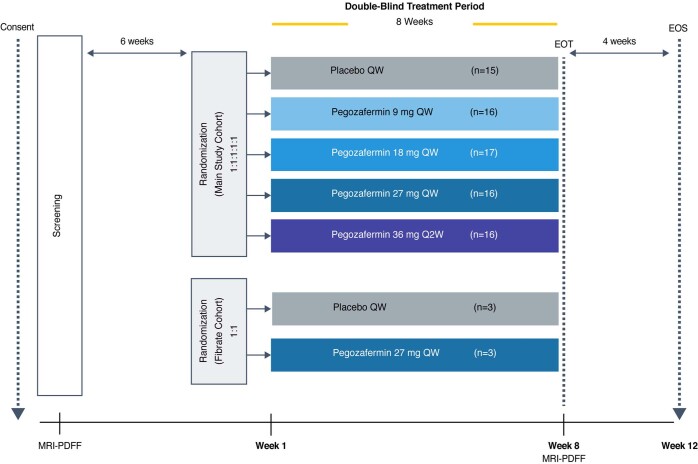
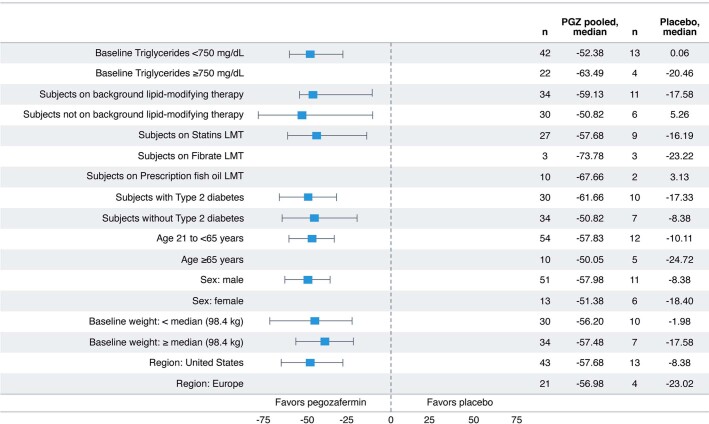
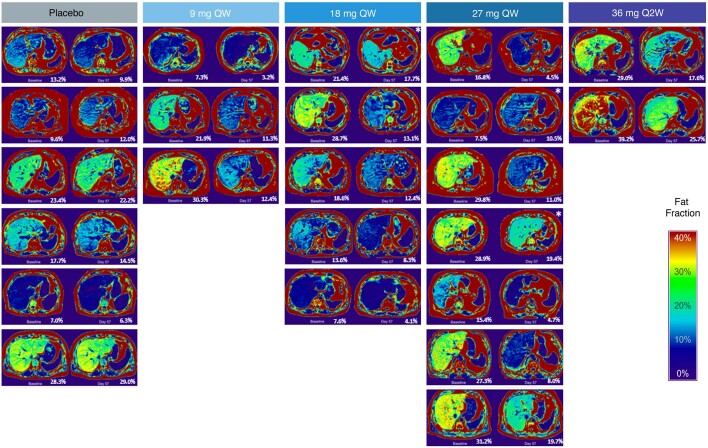
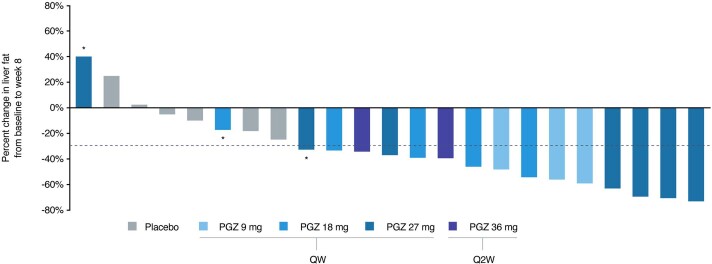
Pegozafermin, a long-acting glycopegylated analog of human fibroblast growth factor 21, is in development for the treatment of severe hypertriglyceridemia (SHTG) and nonalcoholic steatohepatitis. Here we report the results of a phase 2, double-blind, randomized, five-arm trial testing pegozafermin at four different doses (n = 67; 52 male) versus placebo (n = 18; 12 male) for 8 weeks in patients with SHTG (triglycerides (TGs), ≥500 mg dl-1 and ≤2,000 mg dl-1). Treated patients showed a significant reduction in median TGs for the pooled pegozafermin group versus placebo (57.3% versus 11.9%, difference versus placebo -43.7%, 95% confidence interval (CI): -57.1%, -30.3%; P < 0.001), meeting the primary endpoint of the trial. Reductions in median TGs ranged from 36.4% to 63.4% across all treatment arms and were consistent regardless of background lipid-lowering therapy. Results for secondary endpoints included significant decreases in mean apolipoprotein B and non-high-density lipoprotein cholesterol concentrations (-10.5% and -18.3% for pooled doses compared to 1.1% and -0.6% for placebo (95% CI: -21.5%, -2.0%; P = 0.019 and 95% CI: -30.7%, -5.1%; P = 0.007, respectively), as well as a significant decrease in liver fat fraction for pooled treatment (n = 17) versus placebo (n = 6; -42.2% pooled pegozafermin, -8.3% placebo; 95% CI: -60.9%, -8.7%; P = 0.012), as assessed in a magnetic resonance imaging sub-study. No serious adverse events were observed to be related to the study drug. If these results are confirmed in a phase 3 trial, pegozafermin could be a promising treatment for SHTG (ClinicalTrials.gov registration: NCT0441186).
© 2023. The Author(s).
Conflict of interest statement
D.L.B. serves on the following Advisory Boards—AngioWave, Bayer, Boehringer Ingelheim, Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, High Enroll, Janssen, Level Ex, McKinsey, Medscape Cardiology, Merck, MyoKardia, NirvaMed, Novo Nordisk, PhaseBio, PLx Pharma, Regado Biosciences and Stasys. D.L.B. is on the Board of Directors of the following—Angiowave (stock options), Boston VA Research Institute, Bristol Myers Squibb (stock), DRS.LINQ (stock options), High Enroll (stock), Society of Cardiovascular Patient Care and TobeSoft. D.L.B. is the Inaugural Chair of the American Heart Association Quality Oversight Committee. D.L.B. is a Consultant at Broadview Ventures and Hims. D.L.B. is on the following Data Monitoring Committees—Acesion Pharma, Assistance Publique-Hôpitaux de Paris, Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Boston Scientific (Chair, PEITHO trial), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo; for the ABILITY-DM trial, funded by Concept Medical), Novartis, Population Health Research Institute; Rutgers University (for the NIH-funded MINT Trial). D.L.B. has received the following Honoraria—American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Chair, ACC Accreditation Oversight Committee), Arnold and Porter law firm (work related to Sanofi/Bristol Myers Squibb clopidogrel litigation), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor-in-Chief, Harvard Heart Letter), Canadian Medical and Surgical Knowledge Translation Research Group (clinical trial steering committees), Cowen and Company, Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor-in-Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), K2P (Co-Chair, interdisciplinary curriculum), Level Ex, Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Oakstone CME (Course Director, Comprehensive Review of Interventional Cardiology), Piper Sandler, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), WebMD (CME steering committees) and Wiley (steering committee). Additional disclosures for D.L.B. include
Figures
References
-
- Toth PP, et al. High triglycerides are associated with increased cardiovascular events, medical costs, and resource use: a real-world administrative claims analysis of statin-treated patients with high residual cardiovascular risk. J. Am. Heart Assoc. 2018;7:e008740. doi: 10.1161/JAHA.118.008740. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
