

Hypertension in chronic kidney disease-treatment standard 2023
- PMID: 37355779
- PMCID: PMC10689140
- DOI: 10.1093/ndt/gfad118
Hypertension in chronic kidney disease-treatment standard 2023
Abstract
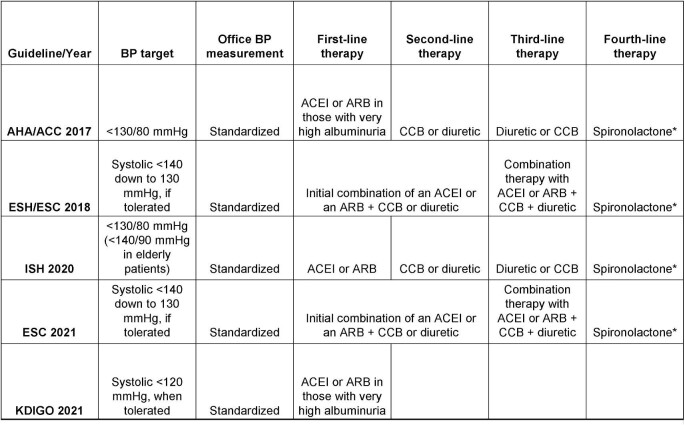
Hypertension is very common and remains often poorly controlled in patients with chronic kidney disease (CKD). Accurate blood pressure (BP) measurement is the essential first step in the diagnosis and management of hypertension. Dietary sodium restriction is often overlooked, but can improve BP control, especially among patients treated with an agent to block the renin-angiotensin system. In the presence of very high albuminuria, international guidelines consistently and strongly recommend the use of an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker as the antihypertensive agent of first choice. Long-acting dihydropyridine calcium channel blockers and diuretics are reasonable second- and third-line therapeutic options. For patients with treatment-resistant hypertension, guidelines recommend the addition of spironolactone to the baseline antihypertensive regimen. However, the associated risk of hyperkalemia restricts the broad utilization of spironolactone in patients with moderate-to-advanced CKD. Evidence from the CLICK (Chlorthalidone in Chronic Kidney Disease) trial indicates that the thiazide-like diuretic chlorthalidone is effective and serves as an alternative therapeutic opportunity for patients with stage 4 CKD and uncontrolled hypertension, including those with treatment-resistant hypertension. Chlorthalidone can also mitigate the risk of hyperkalemia to enable the concomitant use of spironolactone, but this combination requires careful monitoring of BP and kidney function for the prevention of adverse events. Emerging agents, such as the non-steroidal mineralocorticoid receptor antagonist ocedurenone, dual endothelin receptor antagonist aprocitentan and the aldosterone synthase inhibitor baxdrostat offer novel targets and strategies to control BP better. Larger and longer term clinical trials are needed to demonstrate the safety and efficacy of these novel therapies in the future. In this article, we review the current standards of treatment and discuss novel developments in pathophysiology, diagnosis, outcome prediction and management of hypertension in patients with CKD.
Keywords: RAS blockade; chlorthalidone; chronic kidney disease; hypertension; spironolactone.
Published by Oxford University Press on behalf of the ERA 2023.
Conflict of interest statement
R.A. reports personal fees and nonfinancial support from Bayer Healthcare Pharmaceuticals, Akebia Therapeutics, Boehringer Ingelheim, Eli Lilly, Relypsa, Vifor Pharma and Diamedica; is a member of data safety monitoring committees for Vertex and Chinook; has served as an associate editor of the
Figures
Similar articles
-
Management of hypertension in advanced kidney disease.Curr Opin Nephrol Hypertens. 2022 Jul 1;31(4):374-379. doi: 10.1097/MNH.0000000000000812. Curr Opin Nephrol Hypertens. 2022. PMID: 35727171 Free PMC article. Review.
-
Predictors of hyperkalemia risk after hypertension control with aldosterone blockade according to the presence or absence of chronic kidney disease.Nephron Clin Pract. 2014;128(3-4):381-6. doi: 10.1159/000369138. Epub 2015 Jan 6. Nephron Clin Pract. 2014. PMID: 25572273
-
Effects of Spironolactone and Chlorthalidone on Cardiovascular Structure and Function in Chronic Kidney Disease: A Randomized, Open-Label Trial.Clin J Am Soc Nephrol. 2021 Oct;16(10):1491-1501. doi: 10.2215/CJN.01930221. Epub 2021 Aug 30. Clin J Am Soc Nephrol. 2021. PMID: 34462286 Free PMC article. Clinical Trial.
-
Predictors of hyperkalemia risk following hypertension control with aldosterone blockade.Am J Nephrol. 2009;30(5):418-24. doi: 10.1159/000237742. Epub 2009 Sep 9. Am J Nephrol. 2009. PMID: 19738369 Clinical Trial.
-
Low-dose aldosterone blockade as a new treatment paradigm for controlling resistant hypertension.J Clin Hypertens (Greenwich). 2007 Jan;9(1 Suppl 1):19-24. doi: 10.1111/j.1524-6175.2007.06334.x. J Clin Hypertens (Greenwich). 2007. PMID: 17215651 Free PMC article. Review.
Cited by
-
Endogenous bufadienolides, mineralocorticoid receptor antagonists and fibrosis in chronic kidney disease.Front Pharmacol. 2024 Sep 4;15:1431216. doi: 10.3389/fphar.2024.1431216. eCollection 2024. Front Pharmacol. 2024. PMID: 39295945 Free PMC article. Review.
-
Renal denervation is effective in reducing blood pressure in patients with CKD.Clin Kidney J. 2025 Jun 4;18(6):sfaf126. doi: 10.1093/ckj/sfaf126. eCollection 2025 Jun. Clin Kidney J. 2025. PMID: 40491782 Free PMC article. Review.
-
Role of Metformin in Preventing New-Onset Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus.Pharmaceuticals (Basel). 2025 Jan 14;18(1):95. doi: 10.3390/ph18010095. Pharmaceuticals (Basel). 2025. PMID: 39861157 Free PMC article.
-
The role of sex differences in cardiovascular, metabolic, and immune functions in health and disease: a review for "Sex Differences in Health Awareness Day".Biol Sex Differ. 2025 May 13;16(1):33. doi: 10.1186/s13293-025-00714-7. Biol Sex Differ. 2025. PMID: 40361226 Free PMC article. Review.
-
Prevalence, awareness, treatment, and control of hypertension in community-dwelling older adults with chronic kidney disease: the Irish longitudinal study on ageing.Clin Kidney J. 2024 Jun 27;17(8):sfae184. doi: 10.1093/ckj/sfae184. eCollection 2024 Aug. Clin Kidney J. 2024. PMID: 39099566 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
