

Drug combinations identified by high-throughput screening promote cell cycle transition and upregulate Smad pathways in myeloma
- PMID: 37356470
- PMCID: PMC10408729
- DOI: 10.1016/j.canlet.2023.216284
Drug combinations identified by high-throughput screening promote cell cycle transition and upregulate Smad pathways in myeloma
Abstract
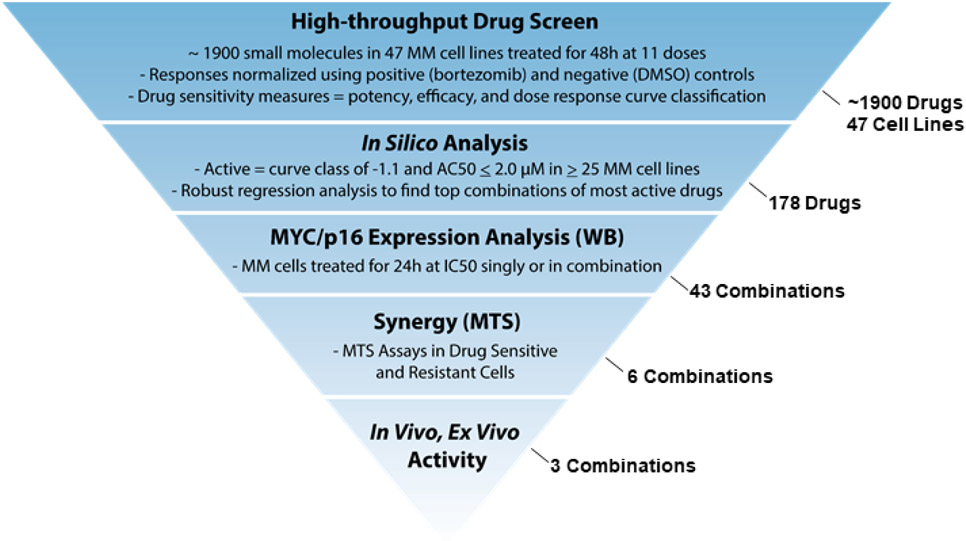
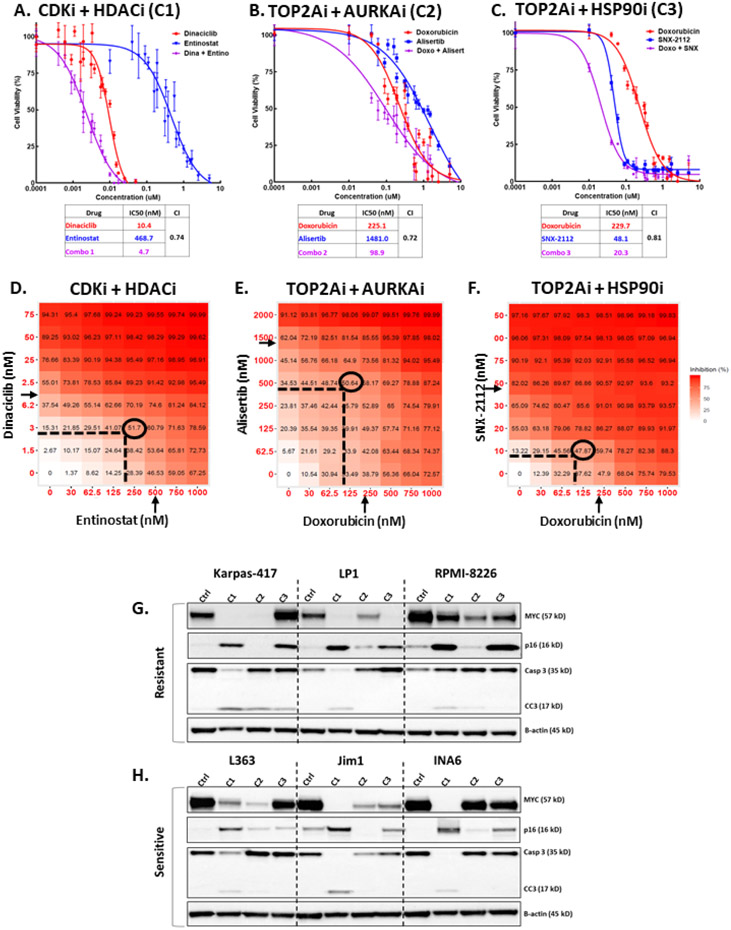
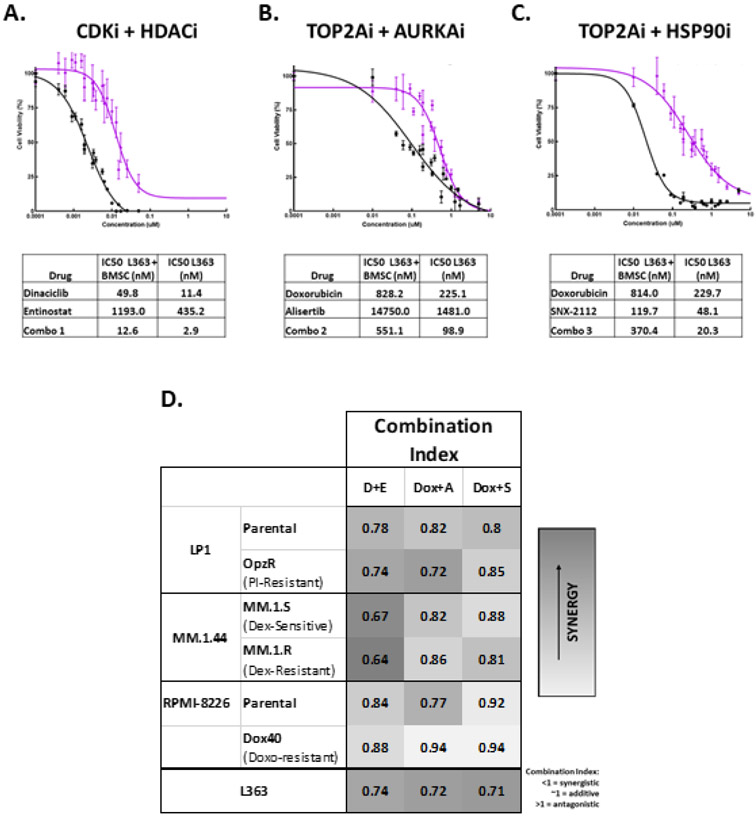
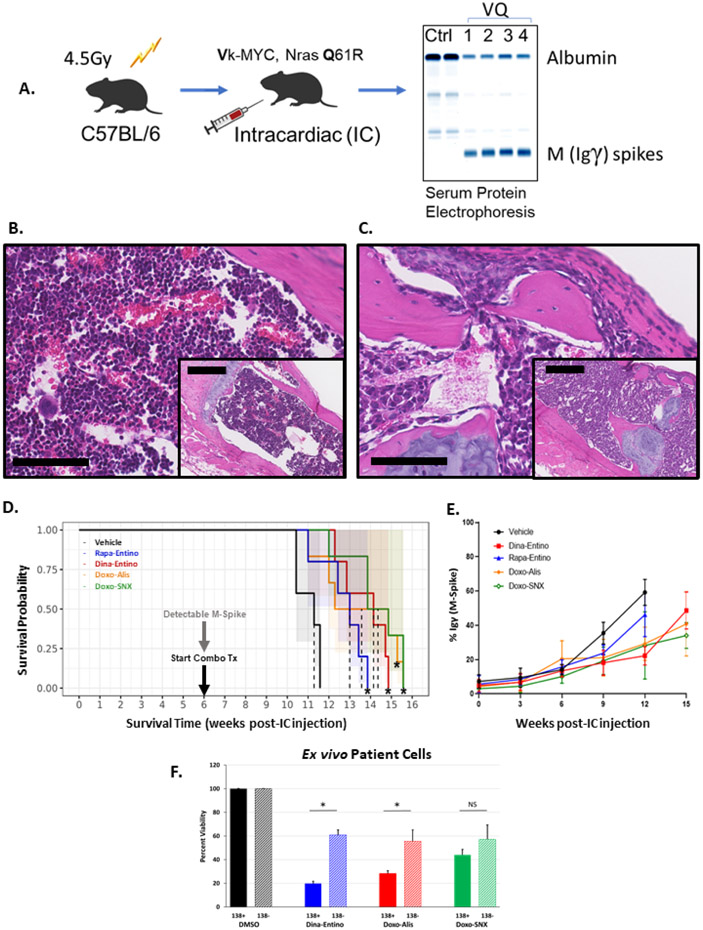
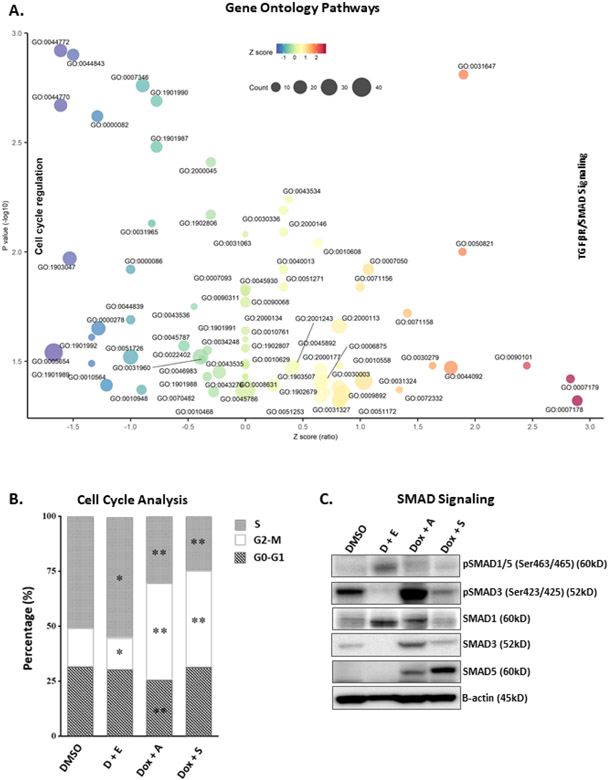
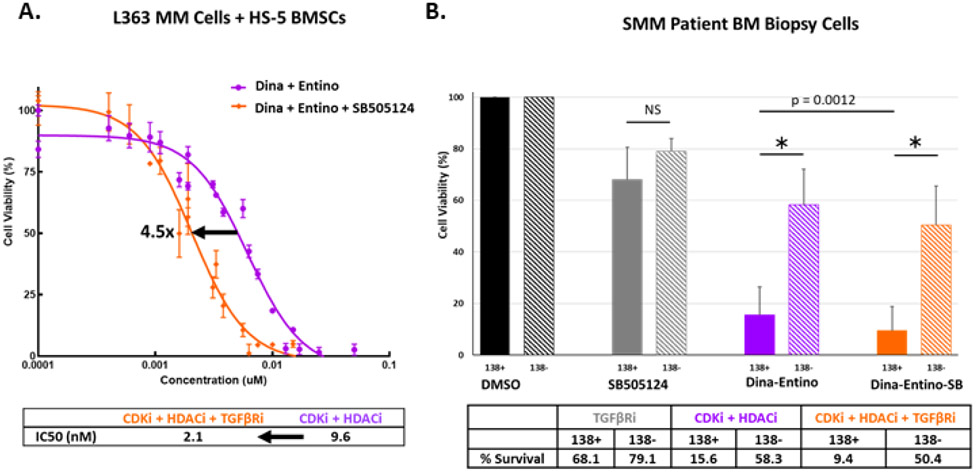
Drug resistance and disease progression are common in multiple myeloma (MM) patients, underscoring the need for new therapeutic combinations. A high-throughput drug screen in 47 MM cell lines and in silico Huber robust regression analysis of drug responses revealed 43 potentially synergistic combinations. We hypothesized that effective combinations would reduce MYC expression and enhance p16 activity. Six combinations cooperatively reduced MYC protein, frequently over-expressed in MM and also cooperatively increased p16 expression, frequently downregulated in MM. Synergistic reductions in viability were observed with top combinations in proteasome inhibitor-resistant and sensitive MM cell lines, while sparing fibroblasts. Three combinations significantly prolonged survival in a transplantable Ras-driven allograft model of advanced MM closely recapitulating high-risk/refractory myeloma in humans and reduced viability of ex vivo treated patient cells. Common genetic pathways similarly downregulated by these combinations promoted cell cycle transition, whereas pathways most upregulated were involved in TGFβ/SMAD signaling. These preclinical data identify potentially useful drug combinations for evaluation in drug-resistant MM and reveal potential mechanisms of combined drug sensitivity.
Keywords: Dinaciclib; Entinostat; MYC; Myeloma; p16.
Copyright © 2023 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Kumar SK, Rajkumar S. The multiple myelomas - current concepts in cytogenetic classification and therapy. Nat Rev Clin Oncol. 2018. Jul;15(7):409–21. - PubMed
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023. Jan;73(1):17–48. - PubMed
-
- Raje N, Berdeja J, Lin Y, Siegel D, Jagannath S, Madduri D, Liedtke M, Rosenblatt J, Maus MV, Turka A, Lam LP, Morgan RA, Friedman K, Massaro M, Wang J, Russotti G, Yang Z, Campbell T, Hege K, Petrocca F, Quigley MT, Munshi N, Kochenderfer JN. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. N Engl J Med. 2019. May 2;380(18):1726–1737. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
