

Evolving spectrum of arrhythmogenic cardiomyopathy: Implications for Sports Cardiology
- PMID: 37357443
- PMCID: PMC10540004
- DOI: 10.1002/clc.24069
Evolving spectrum of arrhythmogenic cardiomyopathy: Implications for Sports Cardiology
Abstract
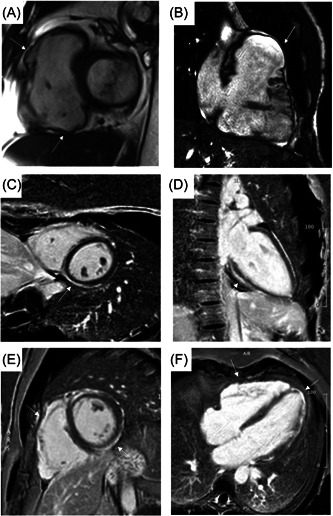
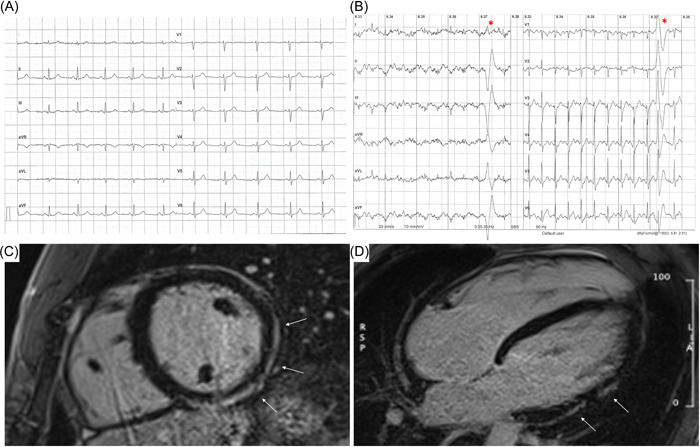
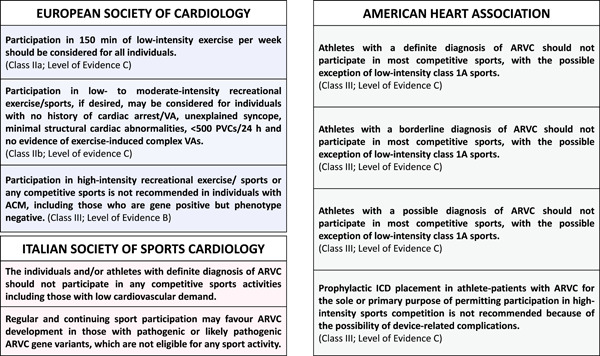
Arrhythmogenic cardiomyopathy (ACM) is a genetic heart muscle disease, structurally characterized by progressive fibro-fatty replacement of the normal myocardium and clinically by ventricular arrhythmias (VAs). Predominantly thanks to the use of cardiac magnetic resonance, we have learnt that the spectrum of the disease encompasses not only the classical right ventricular phenotype, but also biventricular and left dominant variants. Sport activity contributes to the phenotypic expression and progression of ACM and may trigger life-threatening VAs and sudden cardiac death (SCD). We conducted a review of the literature about ACM and its implications in Sport Cardiology and summarized the main findings in this topic. Early identification of affected athletes through preparticipation screening (PPS) is fundamental but, while classical right-ventricular or biventricular phenotypes are usually suspected because of electrocardiogram (ECG) and echocardiographic abnormalities, variants with predominant left ventricular involvement are often characterized by normal ECG and unremarkable echocardiography. Usually the only manifestations of such variants are exercise-induced VAs and for this reason exercise testing may empower the diagnostic yield of the PPS. Patients with ACM are not eligible to competitive sports activity, but low-to-moderate intensity physical activity under medical supervision is possible in most cases.
Keywords: arrhythmogenic cardiomyopathy; athletes; preparticipation screening; sports cardiology; sudden cardiac death.
© 2023 The Authors. Clinical Cardiology published by Wiley Periodicals, LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Corrado D, Link MS, Calkins H. Arrhythmogenic right ventricular cardiomyopathy. N Engl J Med. 2017;376(1):61‐72. - PubMed
-
- Mayosi BM, Fish M, Shaboodien G, et al. Identification of cadherin 2 (CDH2) mutations in arrhythmogenic right ventricular cardiomyopathy. Circ Cardiovasc Genet. 2017;10(2):e001605. - PubMed
-
- van Hengel J, Calore M, Bauce B, et al. Mutations in the area composita protein αT‐catenin are associated with arrhythmogenic right ventricular cardiomyopathy. Eur Heart J. 2013;34(3):201‐210. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
