

Telemedicine for follow-up of systemic lupus erythematosus during the 2019 coronavirus pandemic: A pragmatic randomized controlled trial
- PMID: 37357745
- PMCID: PMC10293868
- DOI: 10.1177/1357633X231181714
Telemedicine for follow-up of systemic lupus erythematosus during the 2019 coronavirus pandemic: A pragmatic randomized controlled trial
Abstract
Introduction: Patients with systemic lupus erythematous were vulnerable to severe coronavirus disease 2019 infection and the negative impact of disrupted healthcare delivery. Telemedicine has been a popular alternative to standard in-person care during the pandemic despite the lack of evidence.
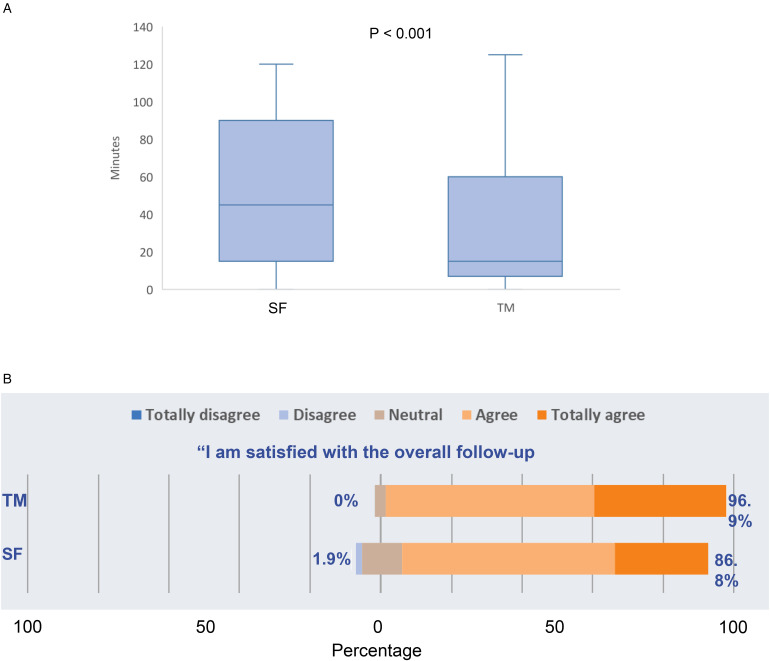
Methods: This was a 1-year pragmatic randomized-controlled trial. Patients followed at the lupus nephritis clinic were randomized to either telemedicine or standard follow-up in a 1:1 ratio. Patients in the telemedicine group were followed up via videoconferencing. Standard follow-up group patients continued conventional in-person outpatient care. The primary outcome of the study was the proportion of patients in low disease activity after 1 year. Secondary outcomes included cost-of-illness, safety, and various patient-reported outcomes.
Results: From 6/2020 to 12/2021, 144 patients were randomized and 141 patients (telemedicine: 70, standard follow-up: 71) completed the study. At 1 year, 80.0% and 80.2% of the patients in the telemedicine group and standard follow-up group were in lupus low disease activity state or complete remission, respectively (p = 0.967). Systemic lupus erythematous disease activity indices, number of flares and frequency of follow-ups were also similar. There were no differences in the cost-of-illness, quality of life or mental health scores. However, significantly more patients in the telemedicine group (41.4% vs 5.6%; p < 0.001) required switch of mode of follow-up and higher proportion of them had hospitalization during the study period (32.9% vs 15.5%; p = 0.016). Being in the telemedicine group or not in low disease activity at baseline were the independent predictors of hospitalization (odds ratio: 2.6; 95% confidence interval: 1.1-6.1, odds ratio: 2.7, 95% confidence interval: 1.1-6.7, respectively) in the post hoc analysis.
Conclusions: In patients with systemic lupus erythematous, telemedicine predominant follow-up resulted in similar 1-year disease control compared to standard care. However, it needed to be complemented by in-person visits, especially in patients with unstable disease.
Keywords: Coronavirus disease 2019; systemic lupus erythematosus; telehealth; telemedicine.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Landewé RB, Machado PM, Kroon F, et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Ann Rheum Dis 2020; 79: 851–858. - PubMed
-
- Mikuls TR, Johnson SR, Fraenkel L, et al. American college of rheumatology guidance for the management of rheumatic disease in adult patients during the COVID-19 pandemic: Version 1. Arthritis Rheumatol 2020; 72: 1241–1251. - PubMed
-
- Ahmed S, Grainger R, Santosa A, et al. APLAR recommendations on the practice of telemedicine in rheumatology. Int J Rheum Dis 2022; 25: 247–258. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
