

Exercise and Experiments of Nature
- PMID: 37358508
- PMCID: PMC10853940
- DOI: 10.1002/cphy.c220027
Exercise and Experiments of Nature
Abstract
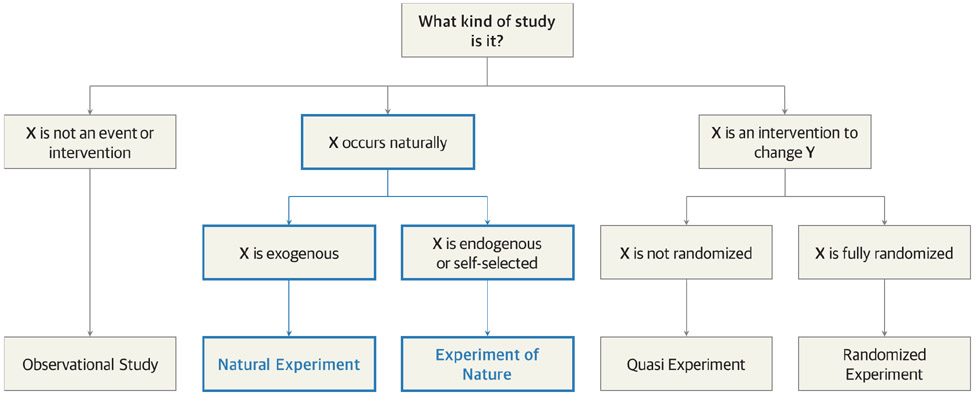
In this article, we highlight the contributions of passive experiments that address important exercise-related questions in integrative physiology and medicine. Passive experiments differ from active experiments in that passive experiments involve limited or no active intervention to generate observations and test hypotheses. Experiments of nature and natural experiments are two types of passive experiments. Experiments of nature include research participants with rare genetic or acquired conditions that facilitate exploration of specific physiological mechanisms. In this way, experiments of nature are parallel to classical "knockout" animal models among human research participants. Natural experiments are gleaned from data sets that allow population-based questions to be addressed. An advantage of both types of passive experiments is that more extreme and/or prolonged exposures to physiological and behavioral stimuli are possible in humans. In this article, we discuss a number of key passive experiments that have generated foundational medical knowledge or mechanistic physiological insights related to exercise. Both natural experiments and experiments of nature will be essential to generate and test hypotheses about the limits of human adaptability to stressors like exercise. © 2023 American Physiological Society. Compr Physiol 13:4879-4907, 2023.
Copyright © 2023 American Physiological Society. All rights reserved.
Figures

References
-
- Adams GR, and Bamman MM. Characterization and regulation of mechanical loading-induced compensatory muscle hypertrophy. Compr Physiol 2: 2829–2870, 2012. - PubMed
-
- Alam M, and Smirk F. Unilateral loss of a blood pressure raising, pulse accelerating, reflex from voluntary muscle due to a lesion of the spinal cord. Clin Sci 3: 247–252, 1938.
-
- American College of Sports Medicine. ACSM's Exercise Testing and Prescription. Wolters Kluwer Health, 2017.
