

Short-Course Therapy for Urinary Tract Infections in Children: The SCOUT Randomized Clinical Trial
- PMID: 37358858
- PMCID: PMC10294016
- DOI: 10.1001/jamapediatrics.2023.1979
Short-Course Therapy for Urinary Tract Infections in Children: The SCOUT Randomized Clinical Trial
Erratum in
-
Errors in Results and Table 2.JAMA Pediatr. 2024 Jun 1;178(6):630. doi: 10.1001/jamapediatrics.2024.0973. JAMA Pediatr. 2024. PMID: 38619852 Free PMC article. No abstract available.
Abstract
Importance: There is a paucity of pediatric-specific comparative data to guide duration of therapy recommendations in children with urinary tract infection (UTI).
Objective: To compare the efficacy of standard-course and short-course therapy for children with UTI.
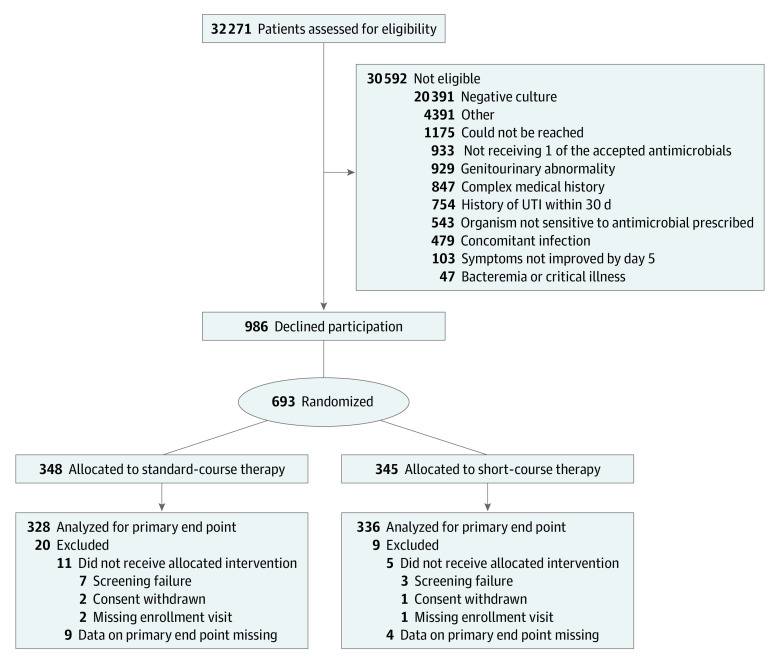
Design, setting, participants: The Short Course Therapy for Urinary Tract Infections (SCOUT) randomized clinical noninferiority trial took place at outpatient clinics and emergency departments at 2 children's hospitals from May 2012, through, August 2019. Data were analyzed from January 2020, through, February 2023. Participants included children aged 2 months to 10 years with UTI exhibiting clinical improvement after 5 days of antimicrobials.
Intervention: Another 5 days of antimicrobials (standard-course therapy) or 5 days of placebo (short-course therapy).
Main outcome measures: The primary outcome, treatment failure, was defined as symptomatic UTI at or before the first follow-up visit (day 11 to 14). Secondary outcomes included UTI after the first follow-up visit, asymptomatic bacteriuria, positive urine culture, and gastrointestinal colonization with resistant organisms.
Results: Analysis for the primary outcome included 664 randomized children (639 female [96%]; median age, 4 years). Among children evaluable for the primary outcome, 2 of 328 assigned to standard-course (0.6%) and 14 of 336 assigned to short-course (4.2%) had a treatment failure (absolute difference of 3.6% with upper bound 95% CI of 5.5.%). Children receiving short-course therapy were more likely to have asymptomatic bacteriuria or a positive urine culture at or by the first follow-up visit. There were no differences between groups in rates of UTI after the first follow-up visit, incidence of adverse events, or incidence of gastrointestinal colonization with resistant organisms.
Conclusions and relevance: In this randomized clinical trial, children assigned to standard-course therapy had lower rates of treatment failure than children assigned to short-course therapy. However, the low failure rate of short-course therapy suggests that it could be considered as a reasonable option for children exhibiting clinical improvement after 5 days of antimicrobial treatment.
Trial registration: ClinicalTrials.gov Identifier: NCT01595529.
Conflict of interest statement
Figures
Comment in
-
Short-Course Therapy for Pediatric Urinary Tract Infections: Evidence-Based Medicine Viewpoint.Indian Pediatr. 2023 Sep 15;60(9):762-764. Indian Pediatr. 2023. PMID: 37705268 No abstract available.
-
Short-Course Therapy for Pediatric Urinary Tract Infections: Pediatrician's Viewpoint.Indian Pediatr. 2023 Sep 15;60(9):765-766. Indian Pediatr. 2023. PMID: 37705270 No abstract available.
-
Nonsuperiority of Standard Therapy Compared to Short-Course Therapy in Symptomatic UTIs.JAMA Pediatr. 2023 Dec 1;177(12):1360-1361. doi: 10.1001/jamapediatrics.2023.4056. JAMA Pediatr. 2023. PMID: 37812426 No abstract available.
Comment on
-
Does the SCOUT Trial Fall Short of Determining an Effective Treatment Duration for Pediatric Urinary Tract Infections?JAMA Pediatr. 2023 Aug 1;177(8):756-758. doi: 10.1001/jamapediatrics.2023.1976. JAMA Pediatr. 2023. PMID: 37358846 No abstract available.
References
-
- Gupta K, Hooton TM, Naber KG, et al. ; Infectious Diseases Society of America; European Society for Microbiology and Infectious Diseases . International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103-e120. doi: 10.1093/cid/ciq257 - DOI - PubMed
