

Investigating the association between neoplasms and MOG antibody-associated disease
- PMID: 37360349
- PMCID: PMC10289293
- DOI: 10.3389/fneur.2023.1193211
Investigating the association between neoplasms and MOG antibody-associated disease
Abstract
Introduction: The association of myelin oligodendrocyte glycoprotein (MOG) antibody associated disease (MOGAD) and tumors has seldom been reported. We aim to investigate the occurrence of tumors in a cohort of patients with MOGAD and to describe their clinical features, in addition to previously reported cases.
Methods: We retrospectively identified patients with MOGAD (i.e., compatible clinical phenotype and positive MOG antibodies analysed with a live cell-based assay) from 1/1/2015 to 1/1/2023 who had a neoplasm diagnosed within 2 years from MOGAD onset. Furthermore, we performed systematic review of literature to identify previously reported cases. Clinical, paraclinical and oncological findings were collected and reported as median (range) or number (percentage).
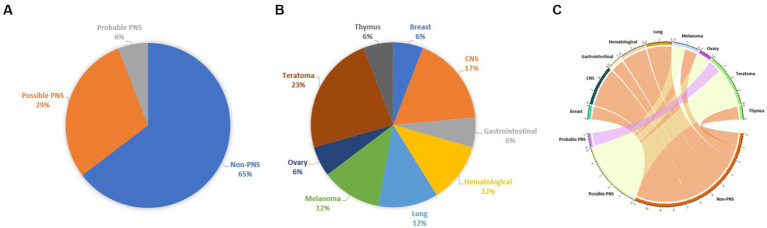
Results: Two of 150 MOGAD patients (1%) had a concomitant neoplasm in our cohort. Fifteen additional cases were retrieved from literature. Median age was 39 (16-73) years-old, 12 patients were female. ADEM (n = 4;23.5%), encephalomyelitis (n = 3;17.6%), and monolateral optic neuritis (n = 2;11.8%) were the most frequent phenotypes. Median number of treatments was 1 (range 1-4), improvement was reported in 14/17 cases (82.4%). Oncological accompaniments were teratoma (n = 4), CNS (n = 3), melanoma (n = 2), lung (n = 2), hematological (n = 2), ovary (n = 1), breast (n = 1), gastrointestinal (n = 1), and thymic (n = 1) neoplasms. Median time from tumor diagnosis to MOGAD onset was 0 (range - 60 to 20) months. MOG expression in neoplastic tissue was reported in 2/4 patients. Median PNS-CARE score was 3 (range 0-7): 11 patients were classified as "non-PNS," 5 as "possible PNS," and 1 as "probable PNS."
Discussion: Our study confirms that MOG is a low-risk antibody for paraneoplastic neurological syndromes and that the clinical presentation and oncological accompaniments are extremely variable. Most of these patients were classified as non-PNS, whereas only a minority was diagnosed with possible/probable PNS, frequently in association with ovarian teratoma. These findings support the notion that MOGAD is not a paraneoplastic disease.
Keywords: cancer; immune checkpoint inhibitors; myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD); paraneoplastic neurological syndrome; tumor.
Copyright © 2023 Trentinaglia, Dinoto, Carta, Chiodega, Ferrari, Andreone, Maniscalco and Mariotto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Dinoto A, Bosco A, Sartori A, Bratina A, Bellavita G, Pasquin F, et al. . Hiccups, severe vomiting and longitudinally extensive transverse myelitis in a patient with prostatic adenocarcinoma and Aquaporin-4 antibodies. J Neuroimmunol. (2021) 352:577488. doi: 10.1016/j.jneuroim.2021.577488, PMID: - DOI - PubMed
-
- Sechi E, Cacciaguerra L, Chen JJ, Mariotto S, Fadda G, Dinoto A, et al. . Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): a review of clinical and MRI features, diagnosis, and management. Front Neurol. (2022) 13:885218. doi: 10.3389/fneur.2022.885218, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources