

Clinical scenarios-based guide for tofacitinib in rheumatoid arthritis
- PMID: 37360417
- PMCID: PMC10286162
- DOI: 10.1177/20406223231178273
Clinical scenarios-based guide for tofacitinib in rheumatoid arthritis
Abstract
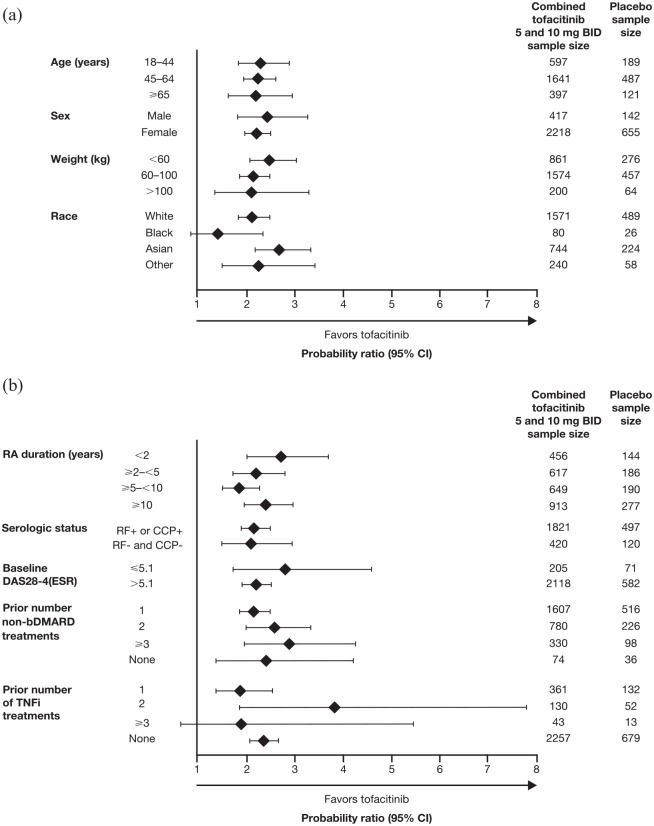
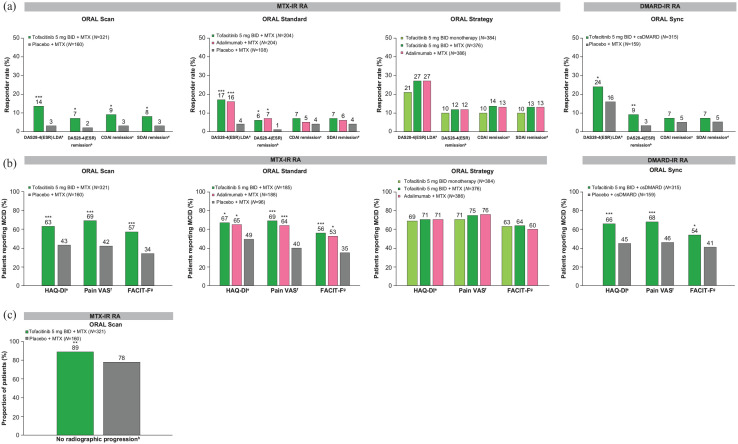
Tofacitinib was the first Janus kinase inhibitor to be approved for the treatment of rheumatoid arthritis (RA), and there is a large body of data to inform the efficacy and safety of this drug for patients at different places in their treatment journeys and with diverse demographics and characteristics. Here, we summarize tofacitinib clinical efficacy and safety data from some clinical trials, post hoc analyses, and real-world studies, which provide evidence of the efficacy of tofacitinib in treating patients with RA at various stages of their treatment journeys, and with differentiating baseline characteristics, such as age, gender, race, and body mass index. In addition, we review the safety data available from different patient subpopulations in the tofacitinib clinical development program, real-world data, and findings from the ORAL Surveillance post-marketing safety study that included patients aged ⩾50 years with pre-existing cardiovascular risk factors. The available efficacy and safety data in these subpopulations can enable better discussions between clinicians and patients to guide informed decision-making and individualized patient care.
Keywords: Janus kinase inhibitors; rheumatoid arthritis; tofacitinib.
© The Author(s), 2023.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MM is an employee and shareholder of Pfizer Inc. EFM is a speaker or advisor to AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Glaxo SmithKline, Janssen, Lilly, Novartis, Pfizer Inc, Roche, and Sanofi.
Figures



References
-
- Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet 2016; 388: 2023–2038. - PubMed
-
- Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 2020; 79: 685–699. - PubMed
-
- Fraenkel L, Bathon JM, England BR, et al. 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 2021; 73: 1108–1123. - PubMed
-
- Lee EB, Fleischmann R, Hall S, et al. Tofacitinib versus methotrexate in rheumatoid arthritis. N Engl J Med 2014; 370: 2377–2386. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
