

A multisociety Delphi consensus statement on new fatty liver disease nomenclature
- PMID: 37363821
- PMCID: PMC10653297
- DOI: 10.1097/HEP.0000000000000520
A multisociety Delphi consensus statement on new fatty liver disease nomenclature
Abstract
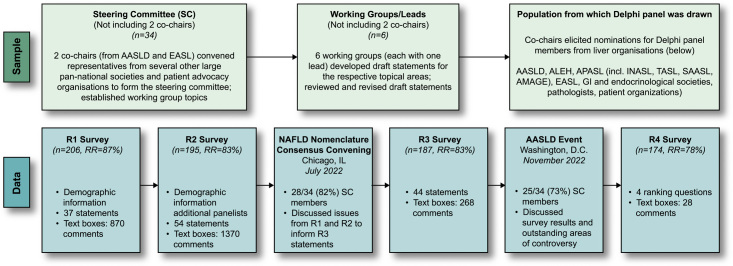
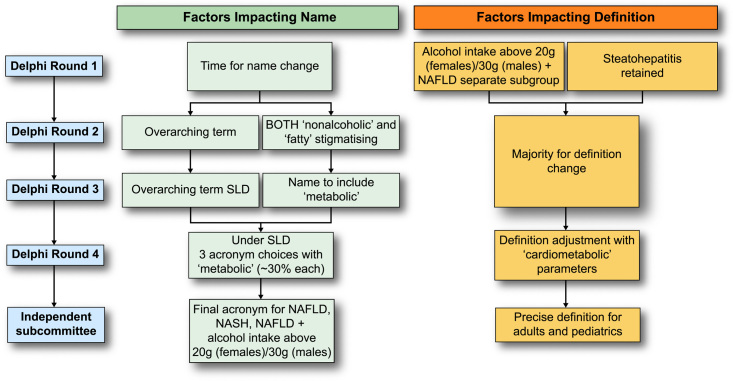
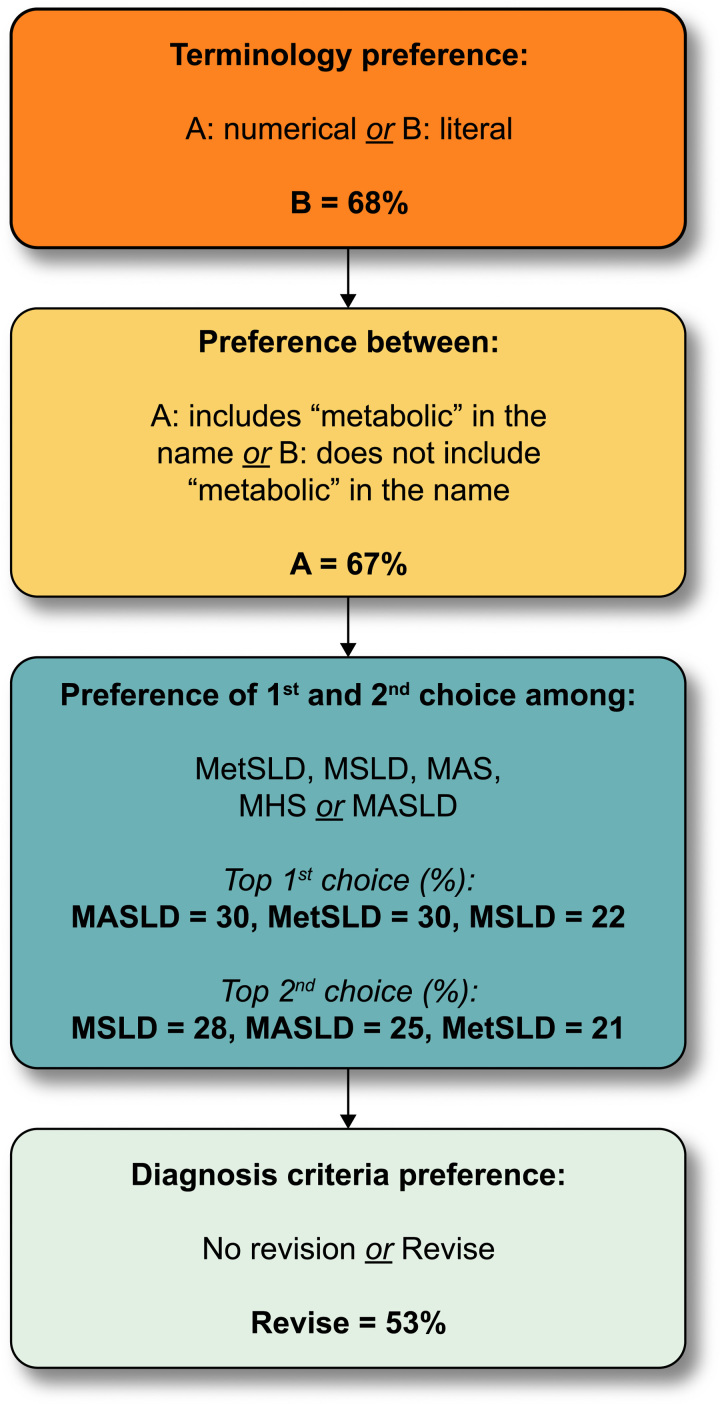
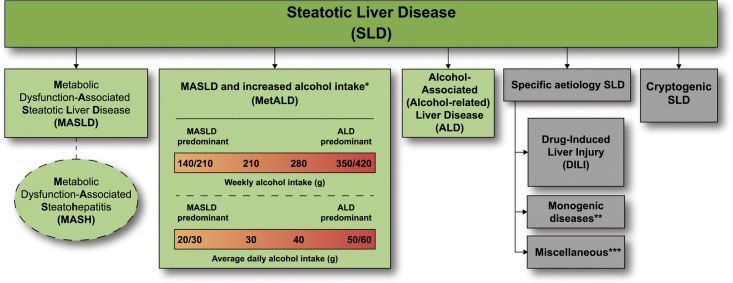
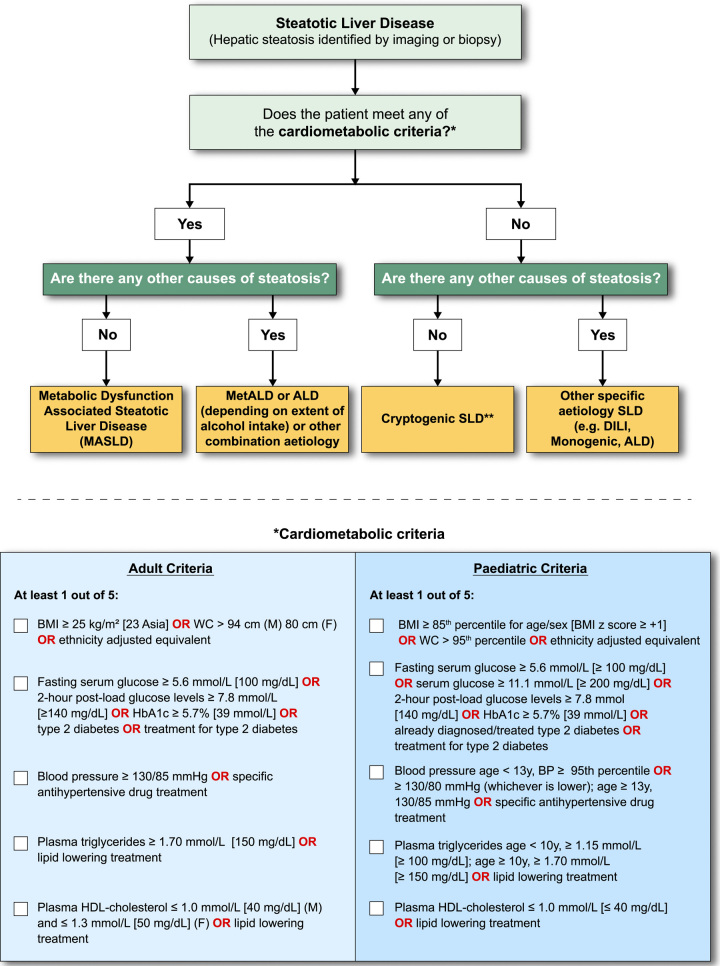
The principal limitations of the terms NAFLD and NASH are the reliance on exclusionary confounder terms and the use of potentially stigmatising language. This study set out to determine if content experts and patient advocates were in favor of a change in nomenclature and/or definition. A modified Delphi process was led by three large pan-national liver associations. The consensus was defined a priori as a supermajority (67%) vote. An independent committee of experts external to the nomenclature process made the final recommendation on the acronym and its diagnostic criteria. A total of 236 panelists from 56 countries participated in 4 online surveys and 2 hybrid meetings. Response rates across the 4 survey rounds were 87%, 83%, 83%, and 78%, respectively. Seventy-four percent of respondents felt that the current nomenclature was sufficiently flawed to consider a name change. The terms "nonalcoholic" and "fatty" were felt to be stigmatising by 61% and 66% of respondents, respectively. Steatotic liver disease was chosen as an overarching term to encompass the various aetiologies of steatosis. The term steatohepatitis was felt to be an important pathophysiological concept that should be retained. The name chosen to replace NAFLD was metabolic dysfunction-associated steatotic liver disease. There was consensus to change the definition to include the presence of at least 1 of 5 cardiometabolic risk factors. Those with no metabolic parameters and no known cause were deemed to have cryptogenic steatotic liver disease. A new category, outside pure metabolic dysfunction-associated steatotic liver disease, termed metabolic and alcohol related/associated liver disease (MetALD), was selected to describe those with metabolic dysfunction-associated steatotic liver disease, who consume greater amounts of alcohol per week (140-350 g/wk and 210-420 g/wk for females and males, respectively). The new nomenclature and diagnostic criteria are widely supported and nonstigmatising, and can improve awareness and patient identification.
Copyright © 2023 American Association for the Study of Liver Disease, European Association for the Study of the Liver (EASL), and Fundación Clínica Médica Sur, A.C. Published by Wolters Kluwer/Elsevier B.V/Elsevier España, S.L.U.
Conflict of interest statement
Manal F. Abdelmalek consults, advises, and received grants from Bristol Myers Squibb, Hanmi, Intercept, Inventiva, and Madrigal. She consults and advises 89Bio, Merck, NGM Bio, Novo Nordisk, Sonic Incytes, and Theratechnologies. She is on the speakers’ bureau for the Chronic Liver Disease Foundation, Clinical Care Options, Fishawack, Medscape, and Terra Firma. She received grants from Allergan, Boehringer Ingelheim, Celgene, Durect, Enanta, Enyo, Galmed, Genentech, Gilead, Novo Nordisk, Poxel, Target NASH, and Viking. Quentin M. Anstee, on behalf of Newcastle University, consults for Alimentiv, Akero, AstraZeneca, Axcella, 89Bio, Boehringer Ingelheim, Bristol Myers Squibb, Galmed, GENFIT, Genentech, Gilead, GSK, Hanmi, HistoIndex, Intercept, Inventiva, Ionis, IQVIA, Janssen, Madrigal, Medpace, Merck, NGM Bio, Novartis, Novo Nordisk, PathAI, Pfizer, Pharmanest, Prosciento, Poxel, RTI, Resolution Therapeutics, Ridgeline Therapeutics, Roche, Shionogi, and Terns. He is on the speakers’ bureau for Fishawack, Integritas Communications, Kenes, Novo Nordisk, Madrigal, Medscape, and Springer Healthcare. He received grants from AstraZeneca, Boehringer Ingelheim, and Intercept. He holds intellectual property rights with Elsevier, Ltd. Ramon Bataller is on the speakers’ bureau for Abbvie and Gilead. Ulrich Beuers consults for CSL Behring. He is on the speakers’ bureau for Abacus and Zambon. Elisabetta Bugianesi advises Boehringer Ingelheim, MSD, and Novo Nordisk. Helena Cortez-Pinto consults and received grants from Novo Nordisk and Roche. She received grants from Eisai, Gilead, GMP-Orphan, and Intercept. Kenneth Cusi Consults for Aligos, Arrowhead, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Covance, Lilly, Madrigal, Myovant, Novo Nordisk, Prosciento, Sagimet, and Siemens. He received grants from Echosens, Inventiva, LabCorp, Nordic Biosciences, and Target NASH. Sven M. Francque consults and received grants from Astellas, Falk, GENFIT, Gilead, Glympse Bio, Janssen, Inventiva, Merck, Pfizer, and Roche. He consults for AbbVie, Actelion, Aelin Therapeutics, Allergan, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Coherus, CSL Behring, Echosens, Eisai, ENYO, Galapagos, Galmed, Genetech, Intercept, Julius Clinical, Madrigal, Medimmune, NGM Bio, Novartis, Novo Nordisk, and Promethera. Samer Gawrieh consults for Pfizer and TransMedics. He received grants from LiverIncytes, Viking, and Zydus. Manuel Romero-Gómez advises and received grants from Novo Nordisk and Siemens. He advises AbbVie, Alpha-sigma, Allergan, AstraZeneca, Axcella, Boehringer Ingelheim, Bristol Myers Squibb, Gilead, Intercept, Inventia, Kaleido, MSD, Pfizer, Prosciento, Rubió, Shionogi, Sobi, and Zydus. He received grants from Echosens and Theratechnologies. Cynthia D. Guy consults for 89Bio, CymaBay, HistoIndex, Madrigal, and NGM. Stephen Harrison consults, advises, is involved with trials, received grants, and owns stock in Akero, Galectin, GENFIT, Hepion, and NGM Bio. He consults, advises, is involved with trials, and received grants from Axcella, Gilead, Intercept, Madrigal, and Poxel. He consults, advises, received grants, and owns stock in NorthSea Therapeutics. He consults, advises, and is involved with trials for Terns. He consults, advises, and received grants from HighTide, Novartis, Novo Nordisk, and Sagimet. He consults, advises, and owns stock in HistoIndex, Metacrine, and Sonic Incytes. He consults, received grants, and owns stock in Cirius. He consults, is involved with trials, and received grants from ENYO and Viking. He is involved with trials and received grants from Genentech. He consults and is involved with trials for Ionis. He consults and received grants from CiVi, CymaBay, Galmed, and Pfizer. He consults and owns stock in Hepta Bio. He consults and advises for Altimmune, Echosens North America, Foresite Labs, and Medpace. He advises and owns stock in ChronWell. He consults for AgomAb, Alentis, Aligos Therapeutics, Alimentiv, Blade, Bluejay, Boston Pharmaceuticals, Boxer Capital, Can-Fite BioPharma, the Chronic Liver Disease Foundation (CLDF), CohBar, Corcept, Fibronostics, Fortress Biotech, Galecto, Gelesis, GSK, GNS Healthcare, GRI Bio, Hepagene, Indalo, Inipharm, Innovate Biopharmaceuticals, Kowa Research Institute, Merck, MGGM, NeuroBo, Nutrasource, Perspectum, Piper Sandler, Prometic (now Liminal BioSciences), Ridgeline Therapeutics, Silverback, and Zafgen (now Larimar). He advises Arrowhead BVF Partners, Humana, and Pathai. He received grants from Bristol Myers Squibb, Conatus, Immuron, and Second Genome. Samuel Klein advises Alnylam, Altimmune, and Merck. Kris V. Kowdley advises, is on the speakers’ bureau, and received grants from Gilead and Intercept. He advises, received grants, and owns stock in Inipharm. He advises and received grants from 89bio, CymaBay, GENFIT, Ipsen, Madrigal, Mirum, NGM Bio, Pfizer, Pliant, and Zeds. He advises Enact, HighTide, and Protagonist. He is on the speakers’ bureau for AbbVie. He received grants from Boston Pharmaceuticals, Corcept, GSK, Hanmi, Janssen, Novo Nordisk, Terns, and Viking. Jeffrey V. Lazarus consults for Novavax. He received grants from AbbVie, Gilead, MSD, and Roche Diagnostics. Rohit Loomba consults and received grants from Arrowhead, AstraZeneca, Bristol Myers Squibb, Galmed, Gilead, Intercept, Inventiva, Ionis, Janssen, Lilly, Madrigal, Merck, NGM Bio, Novo Nordisk, Pfizer, and Terns. He consults and owns stock in 89Bio and Sagimet. Consults for Altimmune, Anylam, Amgen, CohBar, Glympse Bio, HighTide, Inipharm, Metacrine, Novartis, Regeneron, Theratechnologies, and Viking. He received grants from Boehringer Ingelheim, Galectin Therapeutics, Hanmi, and Sonic Incytes. He cofounded and owns stock in LipoNexus. Phillip N. Newsome consults, advises, is on the speakers’ bureau, and received grants from Novo Nordisk. He consults and advises Boehringer Ingelheim, Bristol Myers Squibb, Gilead, GSK, Intercept, Madrigal, Pfizer, Poxel, and Sun Pharma. He is on the speakers’ bureau for AiCME. Elizabeth E. Powell advises and received grants from Novo Nordisk. Vlad Ratziu consults and received grants from Intercept. He consults for Boehringer Ingelheim, Eny, Madrigal, NorthSea, Novo Nordisk, E. Poxel, and Sagimet. He received grants from Gilead. Mary E. Rinella consults for Boehringer Ingelheim, CytoDyn, GSK, Novo Nordisk, HistoIndex, Intercept, Madrigal, NGM Bio, and Sonic Incytes. Michael Roden consults and received grants from Boehringer Ingelheim and Novo Nordisk. He consults for Lilly. He is on the speakers’ bureau for AstraZeneca. Arun J. Sanyal consults and advises Avant Santé and AstraZeneca. He consults and received grants from Akero, Bristol Myers Squibb, Intercept, Lilly, Madrigal, and Novo Nordisk. He consults and owns stock in Rivus. He consults for AGED Diagnostics, Albireo, Alnylam, Altimmune, Boehringer Ingelhiem, 89Bio, Echosense, Genentech, Gilead, GSK, HistoIndex, Malinckrodt, Merck, NGM Bio, Novartis, PathAI, Pfizer, Poxel, Regeneron, Salix, Siemens, Surrozen, Takeda, Terns, and Zydus. He owns stock in Durect, Exhalenz, GENFIT, Indalo, Inversago, and Tiziana. He received royalties from Elsevier and Wolters Kluwer. Marcelo Silva consults, advises, and received grants from Zydus. He received grants from Inventiva and MSD. Dina Tiniakos consults for Clinnovate Health, ICON, Ionis, Inventiva, Merck, and Verily. Luca Valenti consults and received grants from Gilead. He consults for AstraZeneca, Boehringer Ingelheim, MSD, Novo Nordisk, Pfizer, and Resalis Therapeutics. Miriam B. Vos consults and advises Thiogenesis. She consults and received grants from Target Real World Evidence. She consults and owns stock in Intercept. She consults for Albireo, Boehringer Ingelheim, Lilly, Novo Nordisk, and Takeda. She received grants from Bristol Myers Squibb, Quest, and Sonic Incytes. Vincent Wai-Sun Wong consults and received grants from Gilead. He consults for AbbVie, Boehringer Ingelheim, Echosens, Intercept, Inventiva, Novo Nordisk, Pfizer, Sagimet, and TARGET PharmaSolutions. He owns stock in Illuminatio Medical Technology. Yusuf Yilmaz consults for Zydus. He advises Novo Nordisk. He is on the speakers’ bureau for Echosens. Zobair Younossi consults for Bristol Myers Squibb, Gilead, Intercept, Madrigal, Merck, Novartis, Novo Nordisk, Quest, Siemens, and Terns. The remaining authors have no conflicts to report.
Figures
References
-
- Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. 1980;55:434–8. - PubMed
-
- Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–21. - PubMed
-
- Brunt EM. Nonalcoholic steatohepatitis (NASH): further expansion of this clinical entity? Liver. 1999;19:263–4. - PubMed
-
- Bedossa P, Poitou C, Veyrie N, Bouillot JL, Basdevant A, Paradis V, et al. Histopathological algorithm and scoring system for evaluation of liver lesions in morbidly obese patients. Hepatology. 2012;56:1751–9. - PubMed
-
- Matteoni C, Younossi Z, Gramlich T, Boparai N, Liu Y, Mccullough A. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology. 1999;116:1413–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
