

Non-alcoholic fatty liver disease: pathophysiological concepts and treatment options
- PMID: 37364164
- PMCID: PMC10405569
- DOI: 10.1093/cvr/cvad095
Non-alcoholic fatty liver disease: pathophysiological concepts and treatment options
Abstract
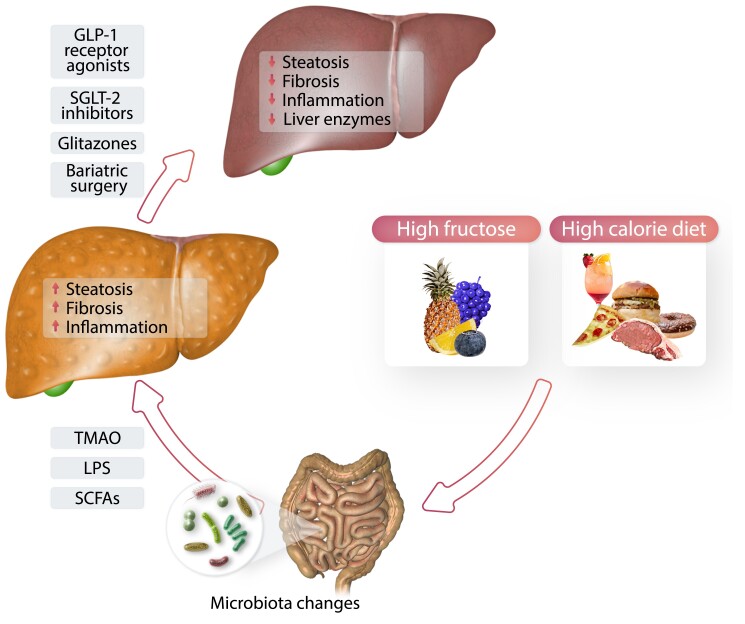
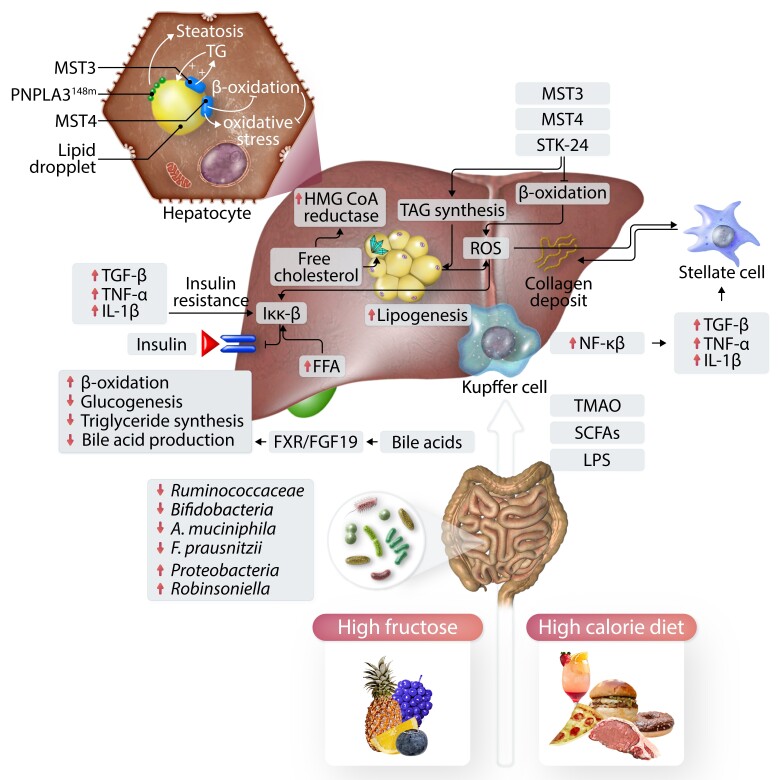
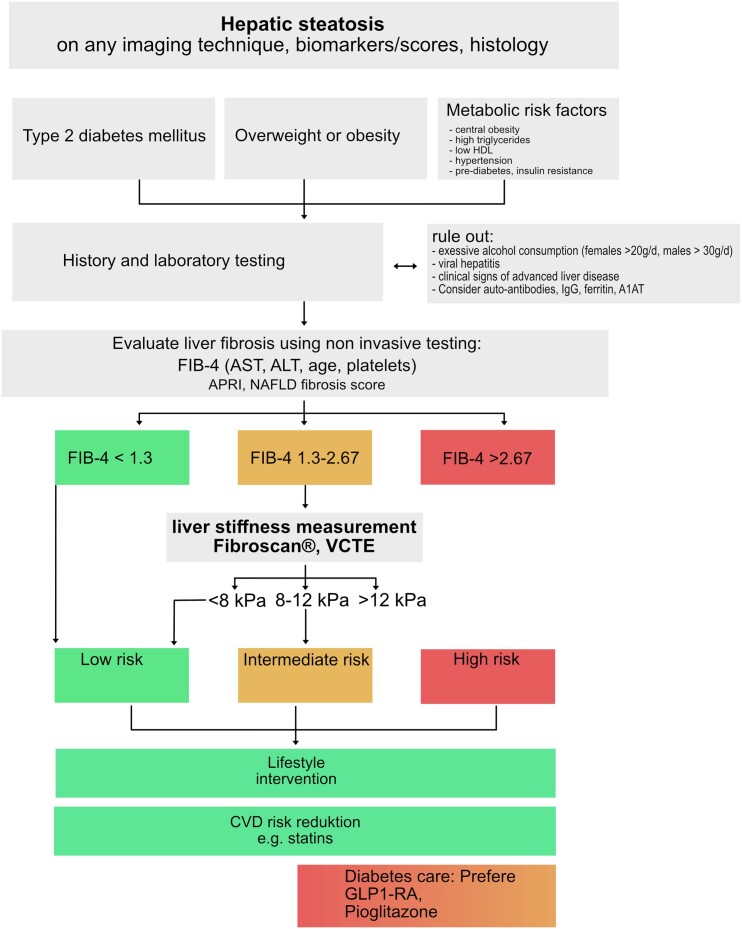
The prevalence of non-alcoholic fatty liver disease (NAFLD) is continually increasing due to the global obesity epidemic. NAFLD comprises a systemic metabolic disease accompanied frequently by insulin resistance and hepatic and systemic inflammation. Whereas simple hepatic steatosis is the most common disease manifestation, a more progressive disease course characterized by liver fibrosis and inflammation (i.e. non-alcoholic steatohepatitis) is present in 10-20% of affected individuals. NAFLD furthermore progresses in a substantial number of patients towards liver cirrhosis and hepatocellular carcinoma. Whereas this disease now affects almost 25% of the world's population and is mainly observed in obesity and type 2 diabetes, NAFLD also affects lean individuals. Pathophysiology involves lipotoxicity, hepatic immune disturbances accompanied by hepatic insulin resistance, a gut dysbiosis, and commonly hepatic and systemic insulin resistance defining this disorder a prototypic systemic metabolic disorder. Not surprisingly many affected patients have other disease manifestations, and indeed cardiovascular disease, chronic kidney disease, and extrahepatic malignancies are all contributing substantially to patient outcome. Weight loss and lifestyle change reflect the cornerstone of treatment, and several medical treatment options are currently under investigation. The most promising treatment strategies include glucagon-like peptide 1 receptor antagonists, sodium-glucose transporter 2 inhibitors, Fibroblast Growth Factor analogues, Farnesoid X receptor agonists, and peroxisome proliferator-activated receptor agonists. Here, we review epidemiology, pathophysiology, and therapeutic options for NAFLD.
Keywords: Cardio vascular disease; Diagnosis; NAFLD; Non-alcoholic liver disease; Pathophysiology; Treatment.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors declare no conflict of interest.
Figures
References
-
- Charlton MR, Burns JM, Pedersen RA, Watt KD, Heimbach JK, Dierkhising RA. Frequency and outcomes of liver transplantation for nonalcoholic steatohepatitis in the United States. Gastroenterology 2011;141:1249–1253. - PubMed
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73–84. - PubMed
-
- Tilg H, Moschen AR, Roden M. NAFLD and diabetes mellitus. Nat Rev Gastroenterol Hepatol 2017;14:32–42. - PubMed
-
- Portillo-Sanchez P, Bril F, Maximos M, Lomonaco R, Biernacki D, Orsak B, Subbarayan S, Webb A, Hecht J, Cusi K. High prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus and normal plasma aminotransferase levels. J Clin Endocrinol Metab 2015;100:2231–2238. - PMC - PubMed
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018;15:11–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
