

The problem of Mycobacterium abscessus complex: multi-drug resistance, bacteriophage susceptibility and potential healthcare transmission
- PMID: 37364635
- PMCID: PMC10583746
- DOI: 10.1016/j.cmi.2023.06.026
The problem of Mycobacterium abscessus complex: multi-drug resistance, bacteriophage susceptibility and potential healthcare transmission
Abstract
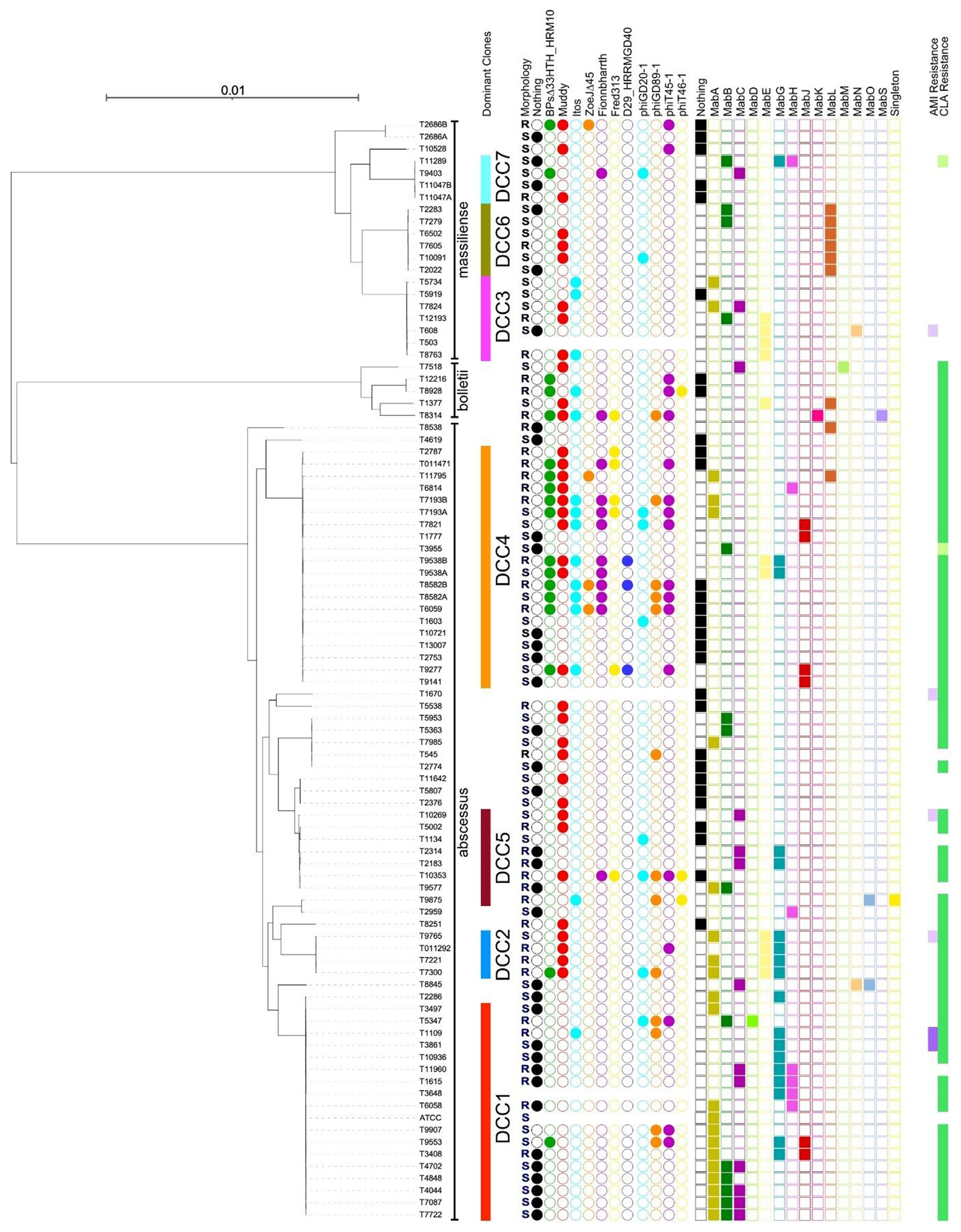
Objectives: Mycobacterium abscessus complex is responsible for 2.6-13.0% of all non-tuberculous mycobacterial pulmonary infections and these are notoriously difficult to treat due to the complex regimens required, drug resistance and adverse effects. Hence, bacteriophages have been considered in clinical practice as an additional treatment option. Here, we evaluated antibiotic and phage susceptibility profiles of M. abscessus clinical isolates. Whole-genome sequencing (WGS) revealed the phylogenetic relationships, dominant circulating clones (DCCs), the likelihood of patient-to-patient transmission and the presence of prophages.
Methods: Antibiotic susceptibility testing was performed using CLSI breakpoints (n = 95), and plaque assays were used for phage susceptibility testing (subset of n = 88, 35 rough and 53 smooth morphology). WGS was completed using the Illumina platform and analysed using Snippy/snp-dists and Discovery and Extraction of Phages Tool (DEPhT).
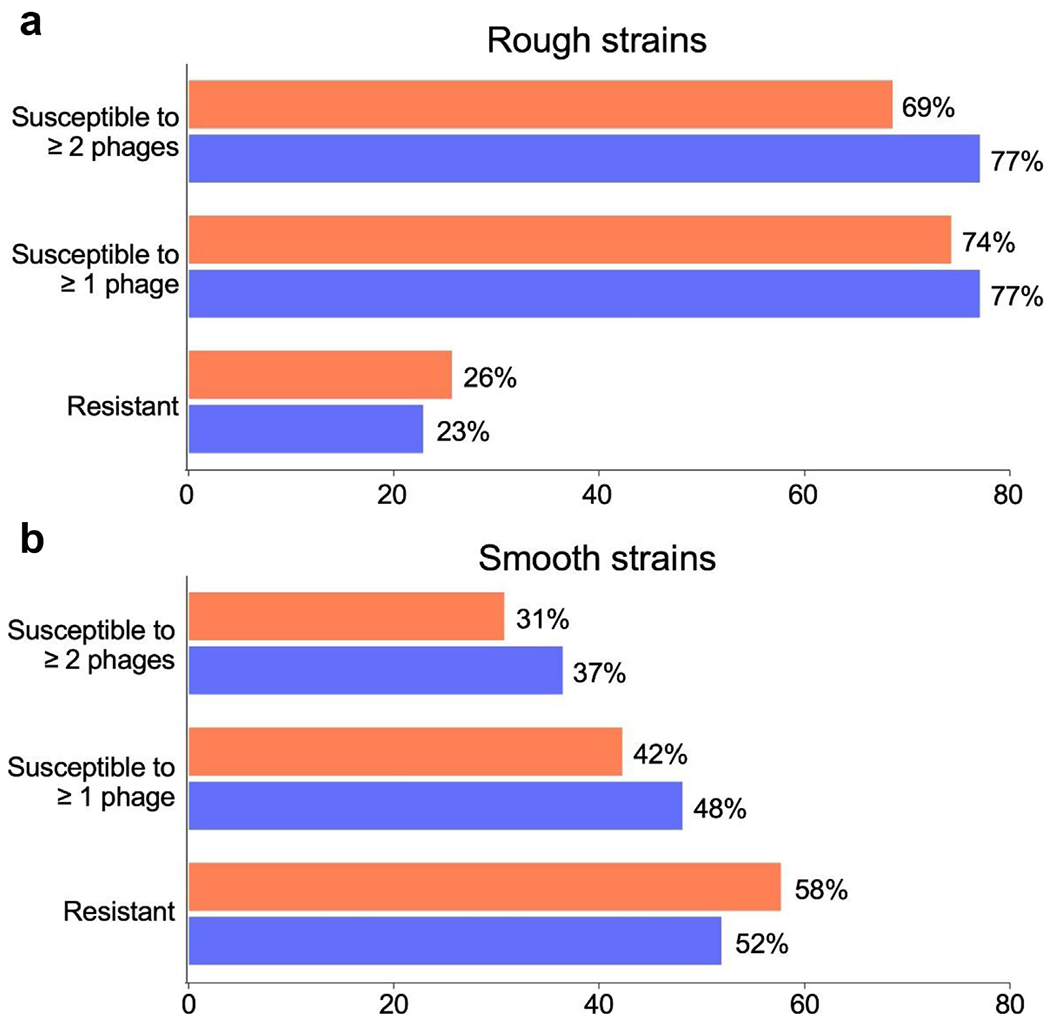
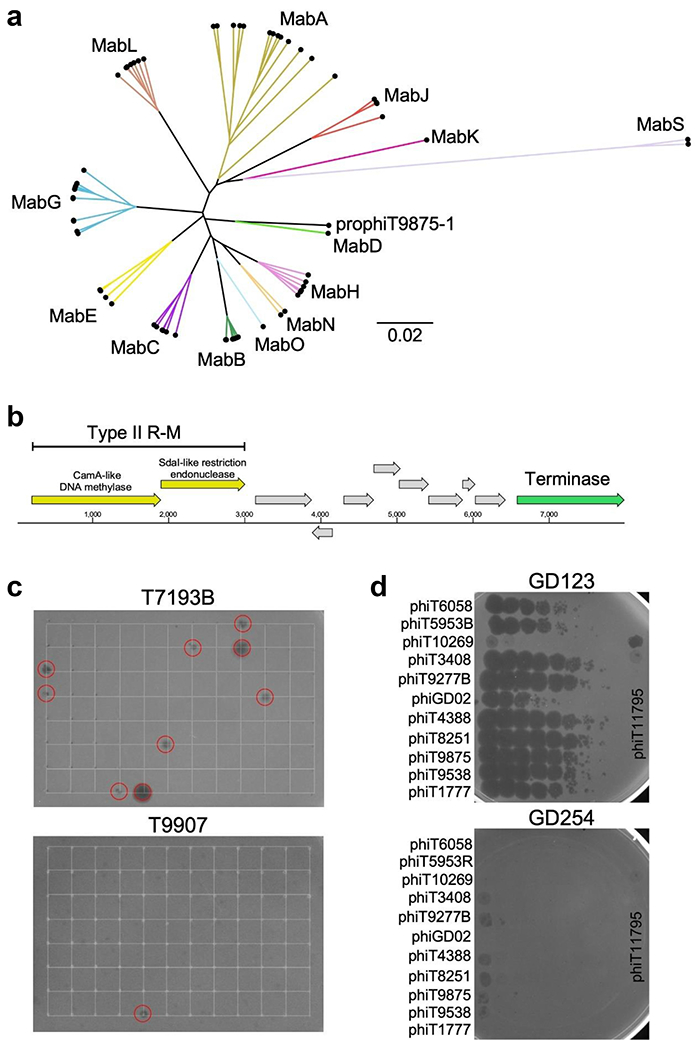
Results: Amikacin and Tigecycline were the most active drugs (with 2 strains resistant to amikacin, and one strain with Tigecycline MIC of 4 μg/mL). Most strains were resistant to all other drugs tested, with Linezolid and Imipenem showing the least resistance, at 38% (36/95) and 55% (52/95), respectively. Rough colony morphotype strains were more phage-susceptible than smooth strains (77%-27/35 versus 48%-25/53 in the plaque assays, but smooth strains are not killed efficiently by those phages in liquid infection assay). We have also identified 100 resident prophages, some of which were propagated lytically. DCC1 (20%-18/90) and DCC4 (22%-20/90) were observed to be the major clones and WGS identified 6 events of possible patient-to-patient transmission.
Discussion: Many strains of M. abscessus complex are intrinsically resistant to available antibiotics and bacteriophages represent an alternative therapeutic option, but only for strains with rough morphology. Further studies are needed to elucidate the role of hospital-borne M. abscessus transmission.
Keywords: Bacteriophages; Multi-drug resistance; Mycobacterium abscessus complex; Next-generation sequencing; Prophages.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
GFH has a Collaborative Research Agreement with Janssen Inc., which did not support the work described here. MRL has provided consulting, participation in advisory board and received lecture fees from Insmed, Savara, Armata, AN2 Therapeutics and 30T. The other authors declare that they have no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
