

Fetal sex and risk of pregnancy-associated malaria in Plasmodium falciparum-endemic regions: a meta-analysis
- PMID: 37365258
- PMCID: PMC10293221
- DOI: 10.1038/s41598-023-37431-3
Fetal sex and risk of pregnancy-associated malaria in Plasmodium falciparum-endemic regions: a meta-analysis
Abstract
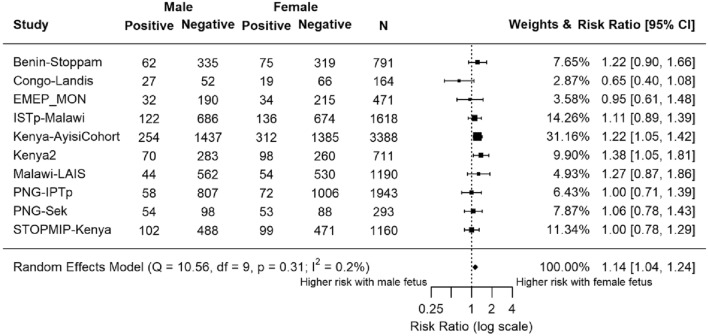
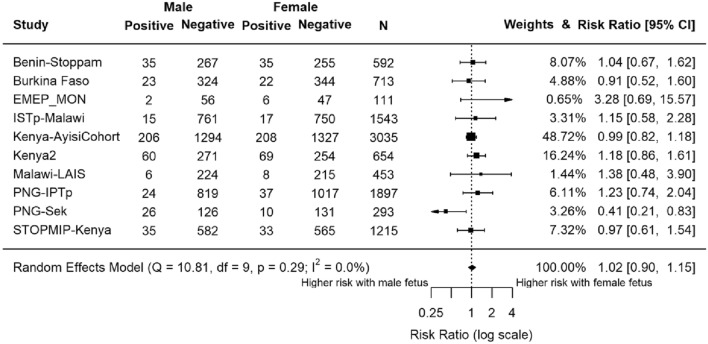
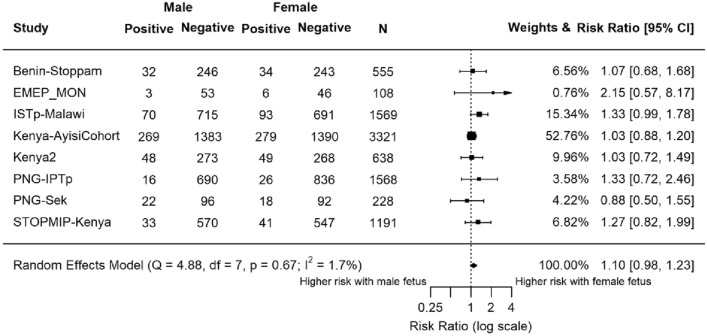
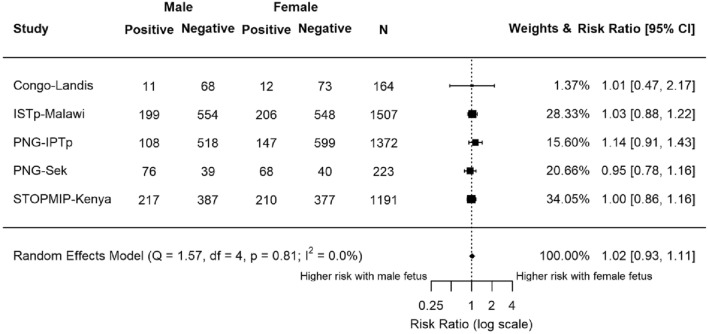
In areas of moderate to intense Plasmodium falciparum transmission, malaria in pregnancy remains a significant cause of low birth weight, stillbirth, and severe anaemia. Previously, fetal sex has been identified to modify the risks of maternal asthma, pre-eclampsia, and gestational diabetes. One study demonstrated increased risk of placental malaria in women carrying a female fetus. We investigated the association between fetal sex and malaria in pregnancy in 11 pregnancy studies conducted in sub-Saharan African countries and Papua New Guinea through meta-analysis using log binomial regression fitted to a random-effects model. Malaria infection during pregnancy and delivery was assessed using light microscopy, polymerase chain reaction, and histology. Five studies were observational studies and six were randomised controlled trials. Studies varied in terms of gravidity, gestational age at antenatal enrolment and bed net use. Presence of a female fetus was associated with malaria infection at enrolment by light microscopy (risk ratio 1.14 [95% confidence interval 1.04, 1.24]; P = 0.003; n = 11,729). Fetal sex did not associate with malaria infection when other time points or diagnostic methods were used. There is limited evidence that fetal sex influences the risk of malaria infection in pregnancy.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript have the following competing interests: SHL is a full-time employee of BioMarin Pharmaceutical and holds shares in BioMarin Pharmaceutical. No other competing interests declared. The findings and conclusions presented in this manuscript are those of the authors and do not reflect the official position of the U.S. Centers for Disease Control and Prevention. JC was funded by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (Pre-doctoral Training in Infectious Disease Epidemiology grant #5 T32 AI070114). HWU is funded through a Menzies School of Health Research Fellowship. The STOPPAM project, “Strategies To Prevent Pregnancy-Associated Malaria”, was supported by the European Union’s Seventh Framework Programme (EU FP7); STOPPAM contract number: 200889. The FSP/MISAME study (Burkina Faso) was funded by Nutrition Third World, The Belgium Ministry of Development, Flemish Interuniversity Council, and French Ministry of Development. The ECHO study (Democratic Republic of the Congo) was funded by the Department of Epidemiology, University of North Carolina Chapel Hill, UNC Gillings School of Global Public Health. EMEP was partly supported by the Malaria in Pregnancy (MiP) Consortium, which was funded through a grant from the Bill & Melinda Gates Foundation to the Liverpool School of Tropical Medicine, UK and partly by the US Centers for Disease Control and Prevention (CDC), Division of Parasitic Diseases and Malaria through a cooperative agreement with Kenya Medical Research Institute (KEMRI), Center for Global Health Research (CGHR), Kisumu, Kenya. The IPTp-MON study (Kenya) was partly supported by the MiP Consortium, which is funded through agrant from the Bill & Melinda Gates Foundation to the Liverpool School of Tropical Medicine, UK and partly supported by the CDC. The ITN project (Kenya) was funded by the US Agency for International Development. The Special Health Support Fund from the Royal Netherlands Embassy (Nairobi, Kenya) provided additional support for the study of the impact of ITN in pregnancy. The Kisumu study (Kenya-2) was funded by US Agency for International Development (grants AOT0483-PH1-2171 and HRN-A-00-04-00010-02) and the Netherlands Foundation for the Advancement of Tropical Research. The STOPMIP study (Kenya) was funded by the Malaria in Pregnancy (MiP) Consortium, which is funded through a grant from the Bill & Melinda Gates Foundation to the Liverpool School of Tropical Medicine, UK. The ISTp study (Malawi) was partly supported by the Malaria in Pregnancy (MiP) Consortium, which is funded through a grant from the Bill & Melinda Gates Foundation to the Liverpool School of Tropical Medicine, UK and partly funded by the European and Developing Countries Clinical Trials Partnership (EDCTP). The LAIS study was supported by grants from the Academy of Finland (Grants 79787 and 207010), the Foundation for Pediatric Research in Finland, and the Medical Research Fund of Tampere University Hospital. Azithromycin and its placebo were provided free of charge by Pfizer Inc (New York, New York), which also provided funding for the polymerase chain reaction testing of the sexually transmitted infections. The IPTp study (Papua New Guinea [PNG]) was funded by the MiP Consortium, through a grant from the Bill & Melinda Gates Foundation (46099); the Pregvax Consortium, through a grant from the EU FP7-2007-HEALTH (PREGVAX 201588) and the Spanish Government (EUROSALUD 2008 Programme); and Pfizer Inc., through an investigator-initiated research grant (WS394663). The Sek study (PNG) was supported by AusAID (grant to PNG Institute of Medical Research [IMR]), the National Health and Medical Research Council of Australia; Australian Research Council; Wellcome Trust; and Veterans Affairs Research Service. The Walter and Eliza Hall Institute is supported by the NHMRC Infrastructure for Research Institutes Support Scheme and Victorian State Government Operational Infrastructure Support. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures
References
-
- WHO . World Malaria Report 2021. World Health Organization; 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
