

Efficacy and safety of isotonic versus hypotonic intravenous maintenance fluids in hospitalized children: an updated systematic review and meta-analysis of randomized controlled trials
- PMID: 37365423
- PMCID: PMC10673968
- DOI: 10.1007/s00467-023-06032-7
Efficacy and safety of isotonic versus hypotonic intravenous maintenance fluids in hospitalized children: an updated systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Iatrogenic hyponatremia is a common complication following intravenous maintenance fluid therapy (IV-MFT) in hospitalized children. Despite the American Academy of Pediatrics' 2018 recommendations, IV-MFT prescribing practices still vary considerably.
Objectives: This meta-analysis aimed to compare the safety and efficacy of isotonic versus hypotonic IV-MFT in hospitalized children.
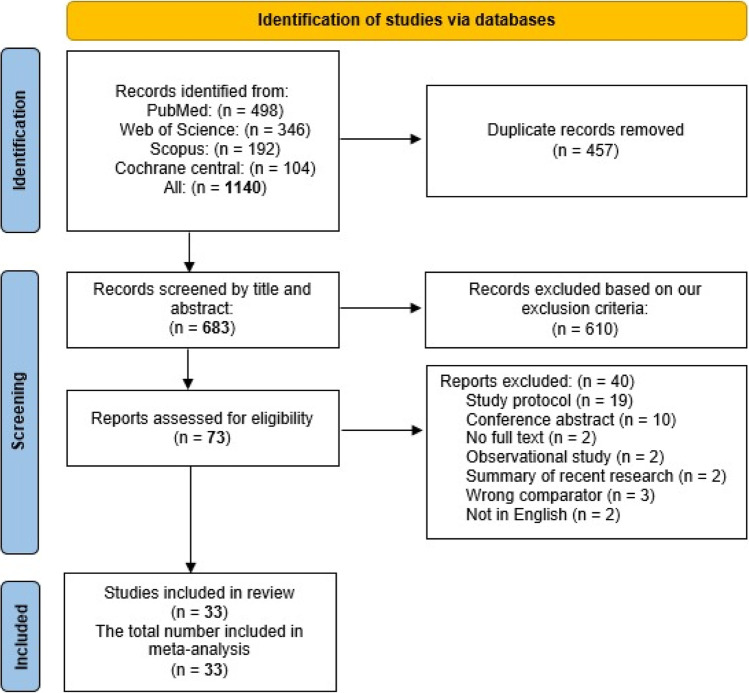
Data sources: We searched PubMed, Scopus, Web of Science, and Cochrane Central from inception to October 1, 2022.
Study eligibility criteria: We included randomized controlled trials (RCTs) comparing isotonic versus hypotonic IV-MFT in hospitalized children, either with medical or surgical conditions. Our primary outcome was hyponatremia following IV-MFT. Secondary outcomes included hypernatremia, serum sodium, serum potassium, serum osmolarity, blood pH, blood sugar, serum creatinine, serum chloride, urinary sodium, length of hospital stay, and adverse outcomes.
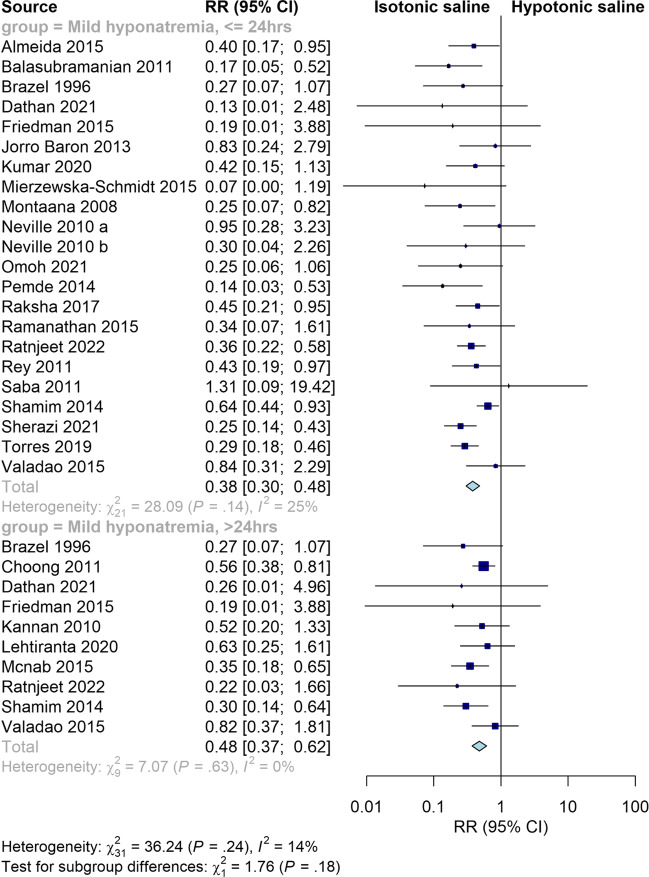
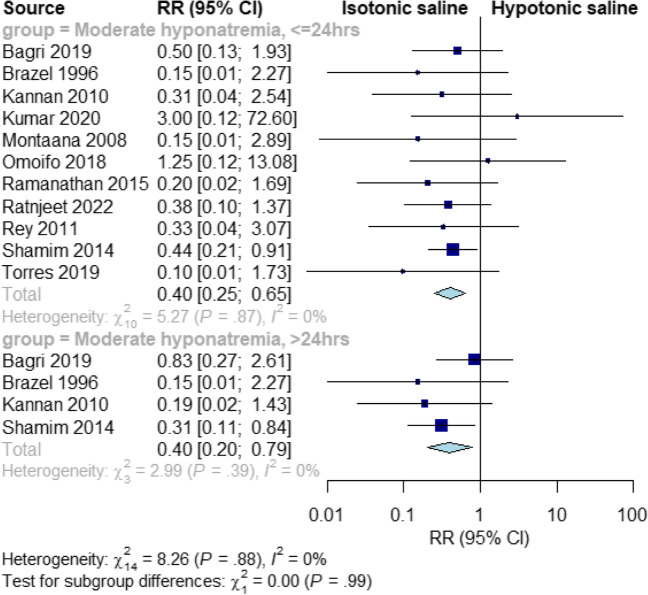
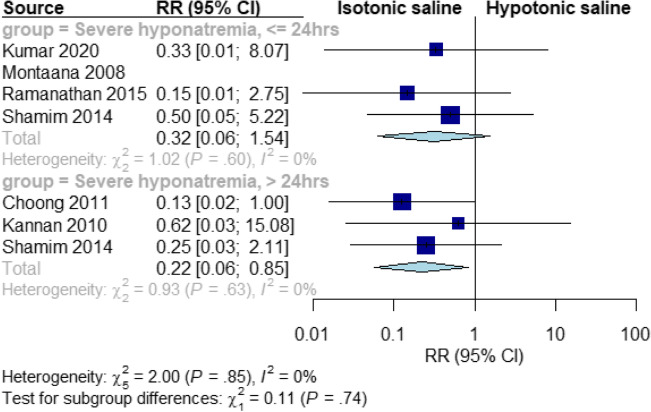
Study appraisal and synthesis methods: Random-effects models were used to pool the extracted data. We performed our analysis based on the duration of fluid administration (i.e., ≤ 24 and > 24 h). The Grades of Recommendations Assessment Development and Evaluation (GRADE) scale was used to evaluate the strength and level of evidence for recommendations.
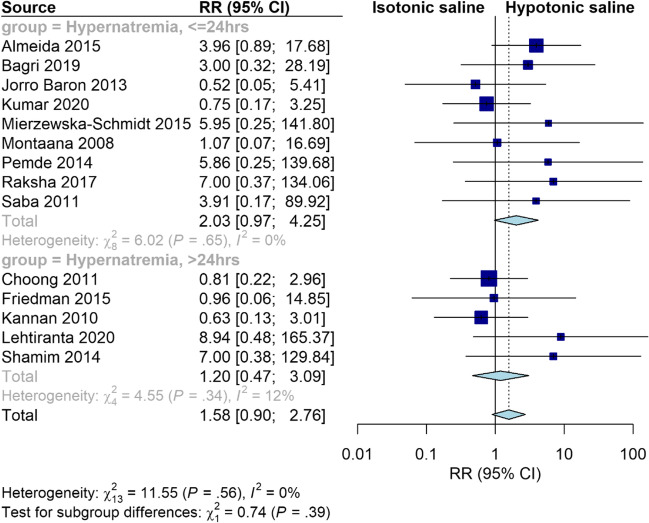
Results: A total of 33 RCTs, comprising 5049 patients were included. Isotonic IV-MFT significantly reduced the risk of mild hyponatremia at both ≤ 24 h (RR = 0.38, 95% CI [0.30, 0.48], P < 0.00001; high quality of evidence) and > 24 h (RR = 0.47, 95% CI [0.37, 0.62], P < 0.00001; high quality of evidence). This protective effect of isotonic fluid was maintained in most examined subgroups. Isotonic IV-MFT significantly increased the risk of hypernatremia in neonates (RR = 3.74, 95% CI [1.42, 9.85], P = 0.008). In addition, it significantly increased serum creatinine at ≤ 24 h (MD = 0.89, 95% CI [0.84, 0.94], P < 0.00001) and decreased blood pH (MD = -0.05, 95% CI [-0.08 to -0.02], P = 0.0006). Mean serum sodium, serum osmolarity, and serum chloride were lower in the hypotonic group at ≤ 24 h. The two fluids were comparable in terms of serum potassium, length of hospital stay, blood sugar, and the risk of adverse outcomes.
Limitations: The main limitation of our study was the heterogeneity of the included studies.
Conclusions and implications of key findings: Isotonic IV-MFT was superior to the hypotonic one in reducing the risk of iatrogenic hyponatremia in hospitalized children. However, it increases the risk of hypernatremia in neonates and may lead to renal dysfunction. Given that the risk of hypernatremia is not important even in the neonates, we propose to use balanced isotonic IV-MFT in hospitalized children as it is better tolerated by the kidneys than 0.9% saline.
Systematic review registration number: CRD42022372359. Graphical abstract A higher resolution version of the Graphical abstract is available as Supplementary information.
Keywords: Children; Hypernatremia; Hyponatremia; Hypotonic; Intravenous fluid; Isotonic.
© 2023. The Author(s).
Conflict of interest statement
All authors have no conflict of interest.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
