

Understanding the age spectrum of respiratory syncytial virus associated hospitalisation and mortality burden based on statistical modelling methods: a systematic analysis
- PMID: 37365569
- PMCID: PMC10294405
- DOI: 10.1186/s12916-023-02932-5
Understanding the age spectrum of respiratory syncytial virus associated hospitalisation and mortality burden based on statistical modelling methods: a systematic analysis
Abstract
Background: Statistical modelling studies based on excess morbidity and mortality are important for understanding RSV disease burden for age groups that are less frequently tested for RSV. We aimed to understand the full age spectrum of RSV morbidity and mortality burden based on statistical modelling studies, as well as the value of modelling studies in RSV disease burden estimation.
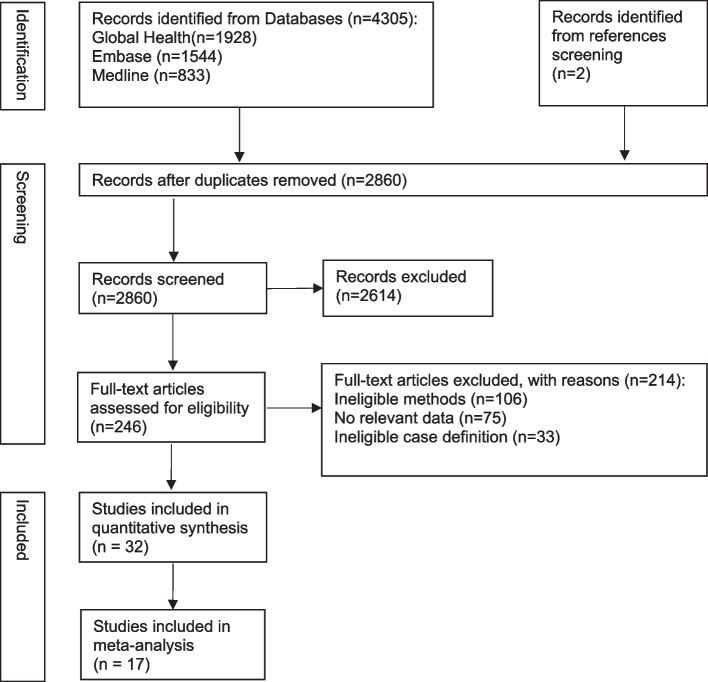
Methods: The databases Medline, Embase and Global Health were searched to identify studies published between January 1, 1995, and December 31, 2021, reporting RSV-associated excess hospitalisation or mortality rates of any case definitions using a modelling approach. All reported rates were summarised using median, IQR (Interquartile range) and range by age group, outcome and country income group; where applicable, a random-effects meta-analysis was conducted to combine the reported rates. We further estimated the proportion of RSV hospitalisations that could be captured in clinical databases.
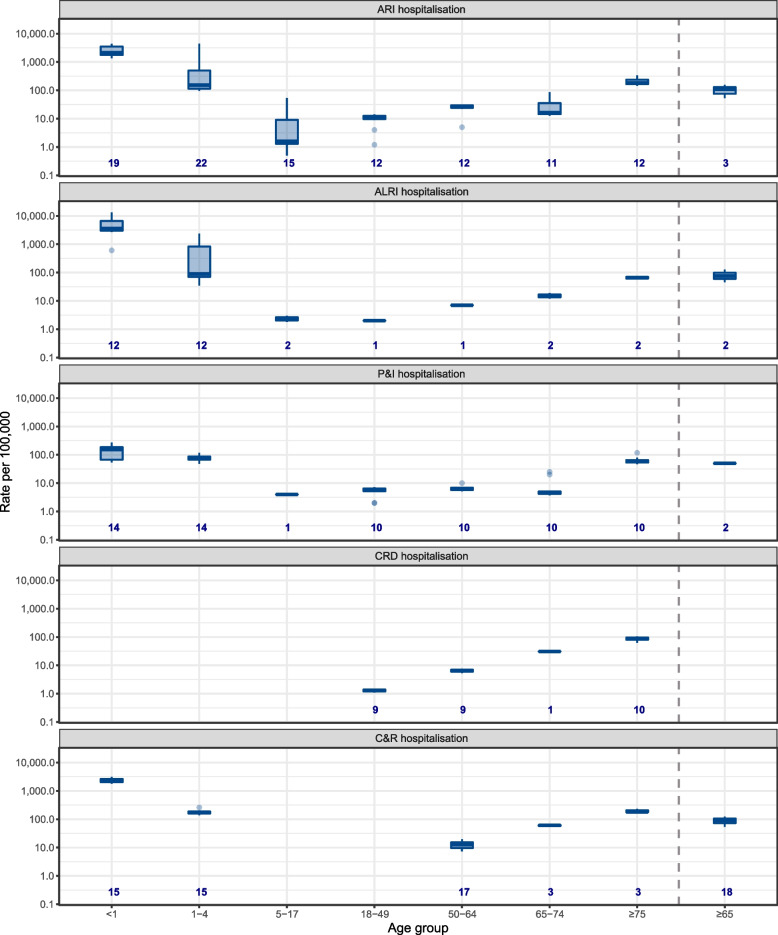
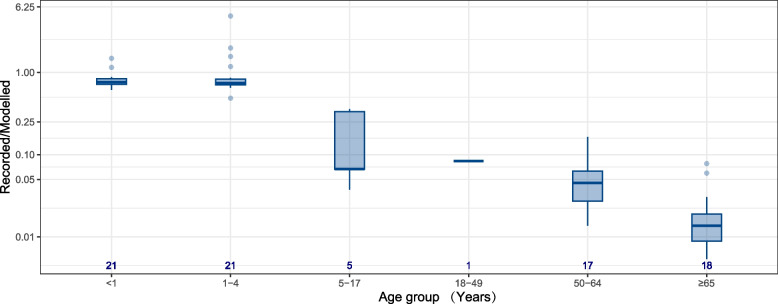
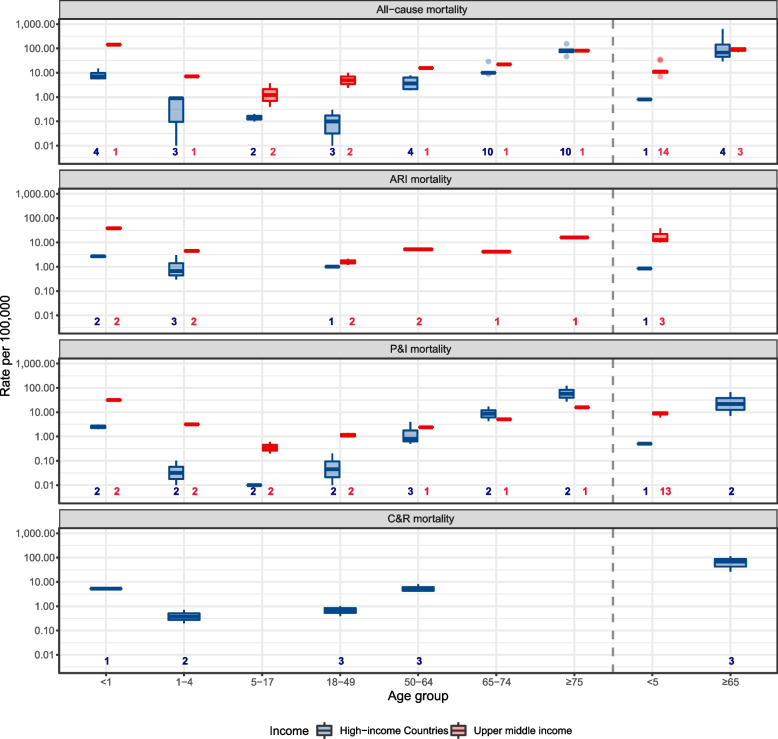
Results: A total of 32 studies were included, with 26 studies from high-income countries. RSV-associated hospitalisation and mortality rates both showed a U-shape age pattern. Lowest and highest RSV acute respiratory infection (ARI) hospitalisation rates were found in 5-17 years (median: 1.6/100,000 population, IQR: 1.3-18.5) and < 1 year (2235.7/100,000 population, 1779.1-3552.5), respectively. Lowest and highest RSV mortality rates were found in 18-49 years (0.1/100,000 population, 0.06-0.2) and ≥ 75 years (80.0/100,000 population, 70.0-90.0) for high-income countries, respectively, and in 18-49 years (0.3/100,000 population, 0.1-2.4) and < 1 year (143.4/100,000 population, 143.4-143.4) for upper-middle income countries. More than 70% of RSV hospitalisations in children < 5 years could be captured in clinical databases whereas less than 10% of RSV hospitalisations could be captured in adults, especially for adults ≥ 50 years. Using pneumonia and influenza (P&I) mortality could potentially capture half of all RSV mortality in older adults but only 10-30% of RSV mortality in children.
Conclusions: Our study provides insights into the age spectrum of RSV hospitalisation and mortality. RSV disease burden using laboratory records alone could be substantially severely underreported for age groups ≥ 5 years. Our findings confirm infants and older adults should be prioritised for RSV immunisation programmes.
Trial registration: PROSPERO CRD42020173430.
Keywords: Burden of disease; Hospitalisation; Model; Mortality; Respiratory syncytial virus; Systematic reviews.
© 2023. The Author(s).
Conflict of interest statement
YL reported grants from the World Health Organization and Wellcome Trust, outside the submitted work. HN reports grants from the Innovative Medicines Initiative outside the submitted work; consulting fees from the Gates Foundation, Pfizer, and Sanofi; honoraria from AbbVie; support from Sanofi for attending meetings; and participation on advisory boards from GSK, Merck, Pfizer, Sanofi, Janssen, Novavax, Reviral, Resvinet, and WHO outside the submitted work. All other authors declared that they have no competing interests.
Figures
References
-
- Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399:2047–2064. doi: 10.1016/S0140-6736(22)00478-0. - DOI - PMC - PubMed
-
- Shi T, Denouel A, Tietjen AK, Campbell I, Moran E, Li X, et al. Global disease burden estimates of respiratory syncytial virus–associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2020;222 Supplement_7:S577–83. doi: 10.1093/infdis/jiz059. - DOI - PubMed
-
- RSV Vaccine and mAb Snapshot | PATH. https://www.path.org/resources/rsv-vaccine-and-mab-snapshot/. Accessed 26 Jul 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
