

Safety and activity of the first-in-class locked nucleic acid (LNA) miR-221 selective inhibitor in refractory advanced cancer patients: a first-in-human, phase 1, open-label, dose-escalation study
- PMID: 37365583
- PMCID: PMC10294514
- DOI: 10.1186/s13045-023-01468-8
Safety and activity of the first-in-class locked nucleic acid (LNA) miR-221 selective inhibitor in refractory advanced cancer patients: a first-in-human, phase 1, open-label, dose-escalation study
Abstract
Background: We developed a 13-mer locked nucleic acid (LNA) inhibitor of miR-221 (LNA-i-miR-221) with a full phosphorothioate (PS)-modified backbone. This agent downregulated miR-221, demonstrated anti-tumor activity against human xenografts in mice, and favorable toxicokinetics in rats and monkeys. Allometric interspecies scaling allowed us to define the first-in-class LNA-i-miR-221 safe starting dose for the clinical translation.
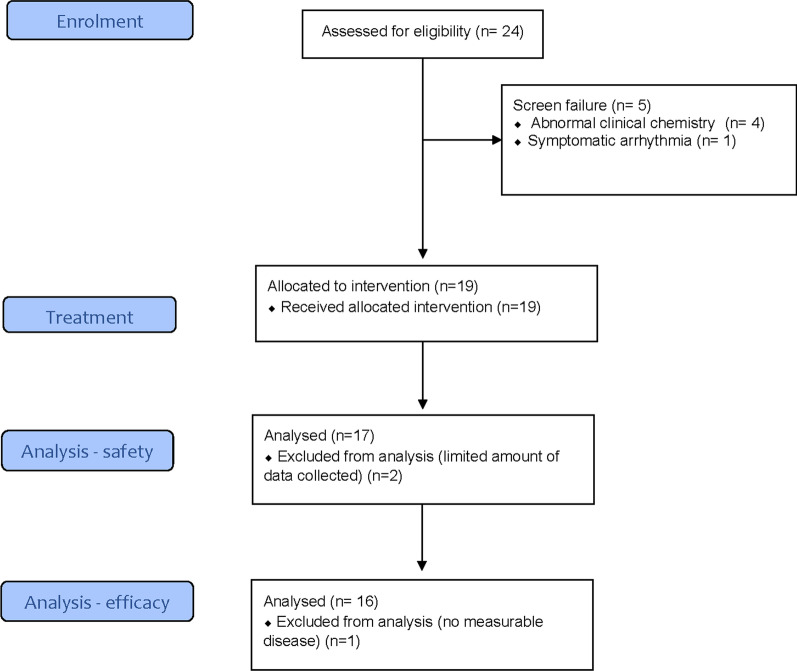
Methods: In this first-in-human, open-label, dose-escalation phase 1 trial, we enrolled progressive cancer patients (aged ≥ 18 years) with ECOG 0-2 into 5 cohorts. The treatment cycle was based on a 30-min IV infusion of LNA-i-miR-221 on 4 consecutive days. Three patients within the first cohort were treated with 2 cycles (8 infusions), while 14 patients were treated with a single course (4 infusions); all patients were evaluated for phase 1 primary endpoint. The study was approved by the Ethics Committee and Regulatory Authorities (EudraCT 2017-002615-33).
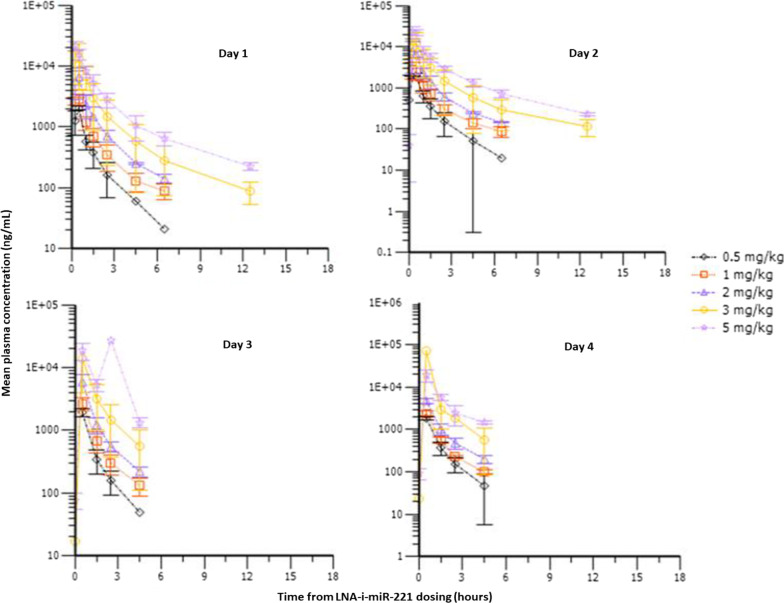
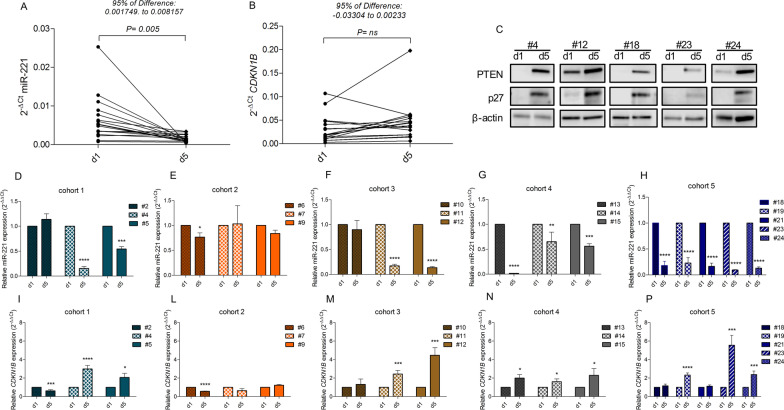
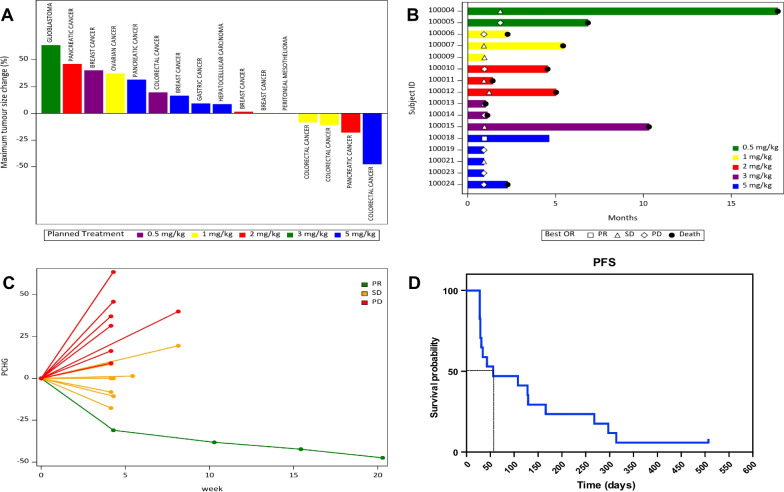
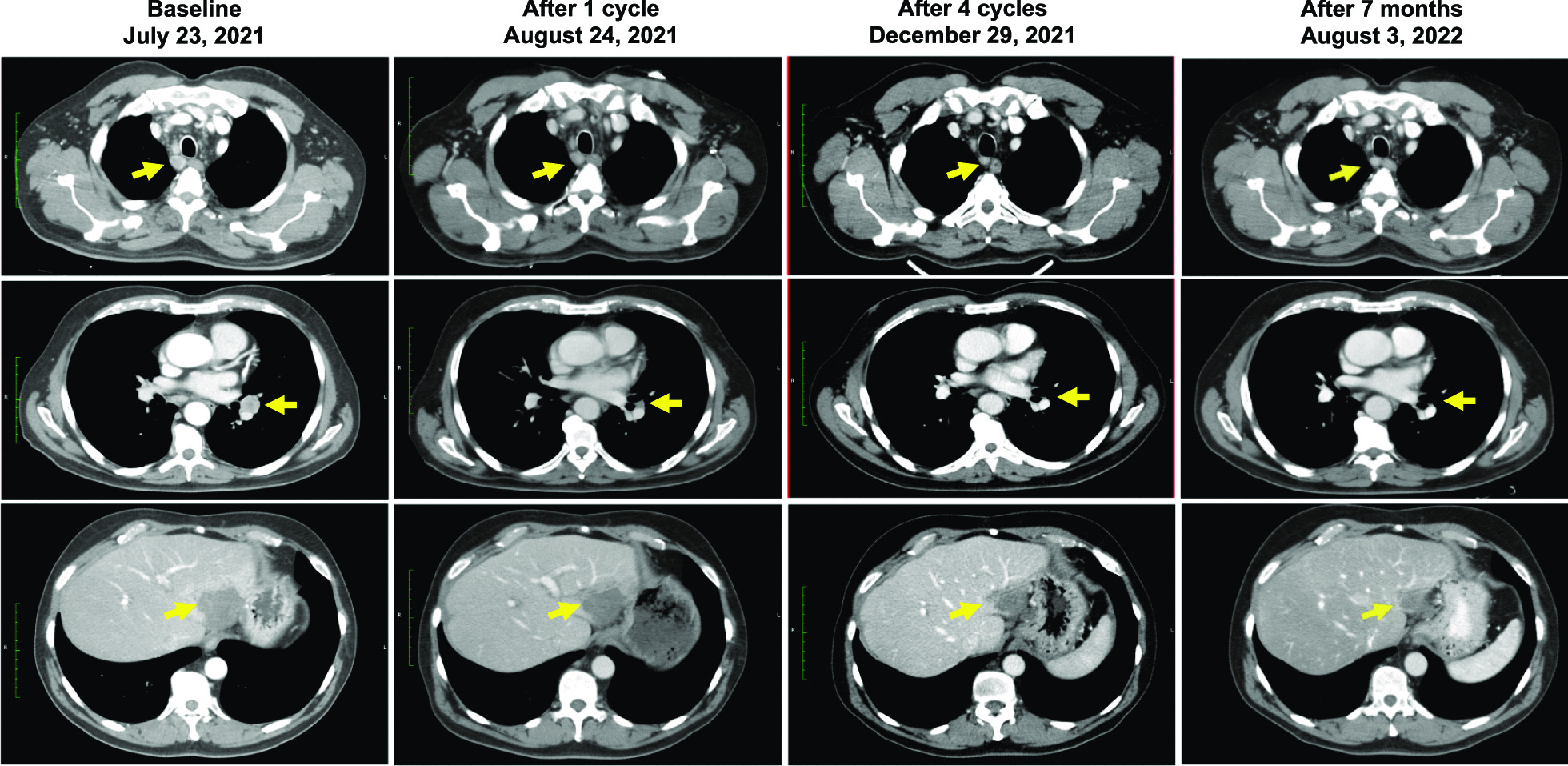
Results: Seventeen patients received the investigational treatment, and 16 were evaluable for response. LNA-i-miR-221 was well tolerated, with no grade 3-4 toxicity, and the MTD was not reached. We recorded stable disease (SD) in 8 (50.0%) patients and partial response (PR) in 1 (6.3%) colorectal cancer case (total SD + PR: 56.3%). Pharmacokinetics indicated non-linear drug concentration increase across the dose range. Pharmacodynamics demonstrated concentration-dependent downregulation of miR-221 and upregulation of its CDKN1B/p27 and PTEN canonical targets. Five mg/kg was defined as the recommended phase II dose.
Conclusions: The excellent safety profile, the promising bio-modulator, and the anti-tumor activity offer the rationale for further clinical investigation of LNA-i-miR-221 (ClinTrials.Gov: NCT04811898).
Keywords: Advanced; Cancer; Clinical trial; First-in-class; First-in-human; LNA-i-miR-221; Non-coding RNA therapeutics; Phase 1; RNA therapeutics; Refractory; miR-221; miRNA; miRNA therapeutics; microRNA.
© 2023. The Author(s).
Conflict of interest statement
P.T., M.T.D.M., and P.T. are inventors of patents (US 9,404,111 B2; EPO 2943570; C.C.I.A.A. 0001429326) that are owned by Magna Graecia University, Catanzaro, Italy. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
