

Endoscopic treatment (endoscopic balloon dilation/self-expandable metal stent) vs surgical resection for the treatment of de novo stenosis in Crohn's disease (ENDOCIR study): an open-label, multicentre, randomized trial
- PMID: 37365665
- PMCID: PMC10294410
- DOI: 10.1186/s13063-023-07447-1
Endoscopic treatment (endoscopic balloon dilation/self-expandable metal stent) vs surgical resection for the treatment of de novo stenosis in Crohn's disease (ENDOCIR study): an open-label, multicentre, randomized trial
Abstract
Background: Stenosis is one of the most common complications in patients with Crohn's disease (CD). Endoscopic balloon dilation (EBD) is the treatment of choice for a short stenosis adjacent to the anastomosis from previous surgery. Self-expandable metal stents (SEMS) may be a suitable treatment option for longer stenoses. To date, however, there is no scientific evidence as to whether endoscopic (EBD/SEMS) or surgical treatment is the best approach for de novo or primary stenoses that are less than 10 cm in length.
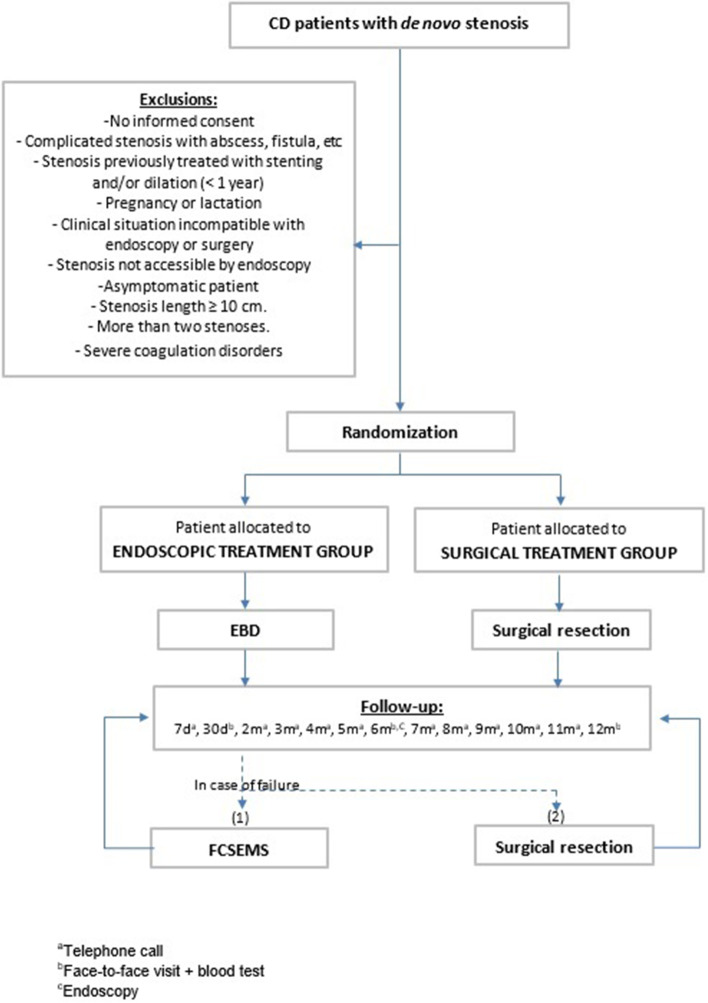
Methods/design: Exploratory study as "proof-of-concept", multicentre, open-label, randomized trial of the treatment of de novo stenosis in the CD; endoscopic treatment (EBD/SEMS) vs surgical resection (SR). The type of endoscopic treatment will initially be with EDB; if a therapeutic failure occurs, then a SEMS will be placed. We estimate 2 years of recruitment and 1 year of follow-up for the assessment of quality of life, costs, complications, and clinical recurrence. After the end of the study, patients will be followed up for 3 years to re-evaluate the variables over the long term. Forty patients with de novo stenosis in CD will be recruited from 15 hospitals in Spain and will be randomly assigned to the endoscopic or surgical treatment groups. The primary aim will be the evaluation of the patient quality of life at 1 year follow-up (% of patients with an increase of 30 points in the 32-item Inflammatory Bowel Disease Questionnaire (IBDQ-32). The secondary aim will be evaluation of the clinical recurrence rate, complications, and costs of both treatments at 1-year follow-up.
Discussion: The ENDOCIR trial has been designed to determine whether an endoscopic or surgical approach is therapeutically superior in the treatment of de novo stenosis in CD.
Trial registration: ClinicalTrials.gov NCT04330846. Registered on 1 April 1 2020. https://clinicaltrials.gov/ct2/home.
Keywords: Balloon dilation; Crohn’s disease; De novo or primary stenosis; Endoscopic treatment; Proof-of-concept study; Randomized clinical trial; Self-expandable metal stent; Surgical resection.
© 2023. The Author(s).
Conflict of interest statement
CL received a speaking fee from Boston Scientific.
JBG is a consultant for Boston Scientific and has received a research grant from Boston Scientific.
DB received speaking fees from Takeda, MSD, Ferring, and Pfizer.
DM Payment or honoraria for lectures, presentations, speaker bureaus, or educational events from Johnson & Johnson. Support for attending meetings and/or travel from Takeda.
FPR is a consultant for Boston Scientific.
FGH is a consultant for Boston Scientific and Ambu.
AV received a speaking fee from Janssen and Tillots Pharma.
ME has received support for conference attendance and research support from Abbvie, Biogen, Faes Farma, Ferring, Jannsen, MSD, Pfizer, Takeda, and Tillotts.
MM has served as a speaker and has received research and an educational grant and advisory fees from AbbVie, Takeda, Pfizer, Janssen, Galapagos, and Ferring.
MMBW declares educational activities, research projects, scientific meetings, and advisory boards sponsored by MSD, Ferring, Abbvie, Janssen, Biogen, and Takeda.
VP is a consultant for Boston Scientific.
JG has served as a speaker, consultant, and advisory member for or has received research funding from Roche, MSD, Abbvie, Kern Pharma, Takeda, Janssen, Pfizer, Ferring, Chiesi, Galapagos, Sandoz, Celltrion, and GE Healthcare.
The other authors declare that they have no competing interests.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
