

Global, Regional, and National Advances Toward the Management of Rheumatic Heart Disease Based on the Global Burden of Disease Study 2019
- PMID: 37366108
- PMCID: PMC10356074
- DOI: 10.1161/JAHA.122.028921
Global, Regional, and National Advances Toward the Management of Rheumatic Heart Disease Based on the Global Burden of Disease Study 2019
Abstract
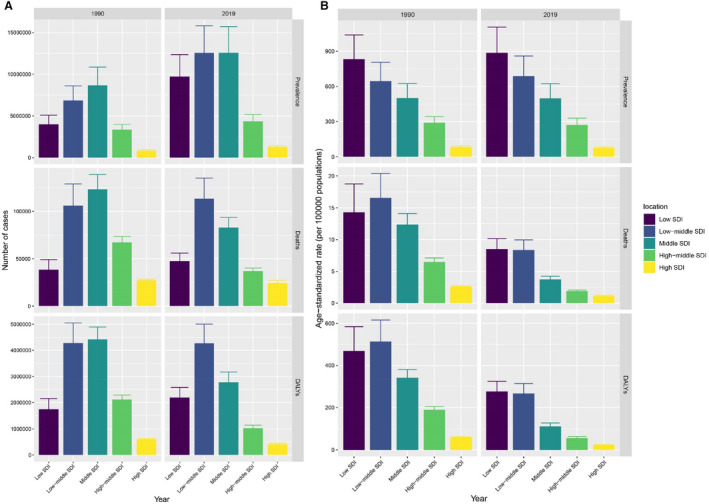
Background Population growth, aging, and major alterations in epidemiologic trends inadvertently modulate the status of rheumatic heart disease (RHD) epidemiology. This investigation predicted RHD burden pattern and temporal trends to provide epidemiologic evidence. Methods and Results Prevalence, mortality, and disability-adjusted life-years data for RHD were obtained from the GBD (Global Burden of Disease) study. We performed decomposition analysis and frontier analysis to assess variations and burden in RHD from 1990 to 2019. In 2019, there were >40.50 million RHD cases worldwide, along with nearly 0.31 million RHD-related deaths and 10.67 million years of healthy life lost to RHD. The RHD burden was commonly concentrated within lower sociodemographic index regions and countries. RHD primarily affects women (22.52 million cases in 2019), and the largest age-specific prevalence rate was at 25 to 29 years in women and 20 to 24 years in men. Multiple reports demonstrated prominent downregulation of RHD-related mortality and disability-adjusted life-years at the global, regional, and national levels. Decomposition analysis revealed that the observed improvements in RHD burden were primarily due to epidemiological alteration; however, it was negatively affected by population growth and aging. Frontier analysis revealed that the age-standardized prevalence rates were negatively linked to sociodemographic index, whereas Somalia and Burkina Faso, with lower sociodemographic index, showed the lowest overall difference from the frontier boundaries of mortality and disability-adjusted life-years. Conclusions RHD remains a major global public health issue. Countries such as Somalia and Burkina Faso are particularly successful in managing adverse outcomes from RHD and may serve as a template for other countries.
Keywords: Global Burden of Disease 2019; disability‐adjusted life‐years; mortality; prevalence; rheumatic heart disease.
Figures




References
-
- Rothenbühler M, O'Sullivan CJ, Stortecky S, Stefanini GG, Spitzer E, Estill J, Shrestha NR, Keiser O, Jüni P, Pilgrim T. Active surveillance for rheumatic heart disease in endemic regions: a systematic review and meta‐analysis of prevalence among children and adolescents. Lancet Glob Health. 2014;2:e717–e726. doi: 10.1016/S2214-109X(14)70310-9 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
