

A Multicenter Assessment of Interreader Reliability of LI-RADS Version 2018 for MRI and CT
- PMID: 37367445
- PMCID: PMC10315518
- DOI: 10.1148/radiol.222855
A Multicenter Assessment of Interreader Reliability of LI-RADS Version 2018 for MRI and CT
Erratum in
-
Erratum for: A Multicenter Assessment of Interreader Reliability of LI-RADS Version 2018 for MRI and CT.Radiology. 2023 Jul;308(1):e239018. doi: 10.1148/radiol.239018. Radiology. 2023. PMID: 37489994 Free PMC article. No abstract available.
Abstract
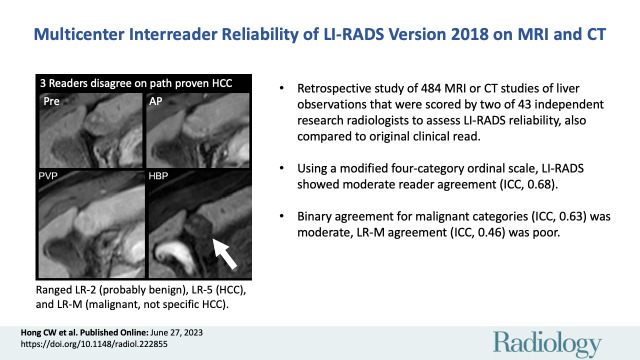
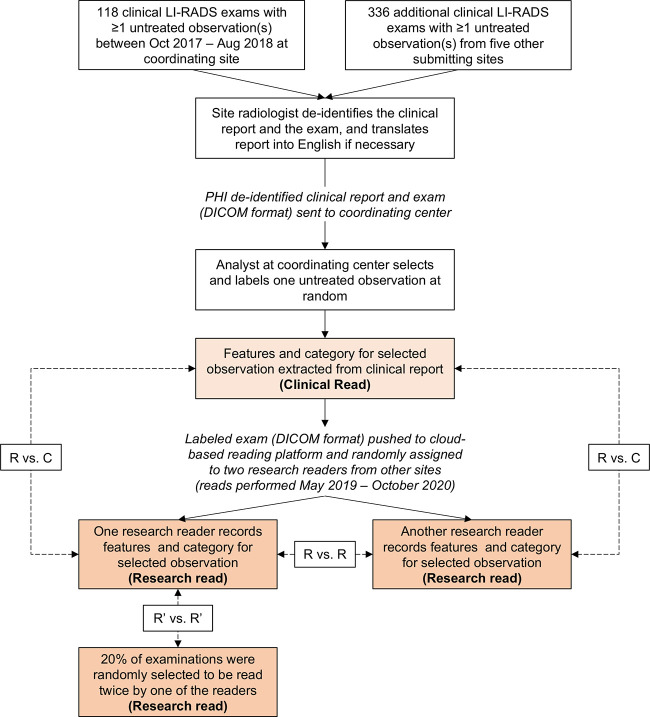
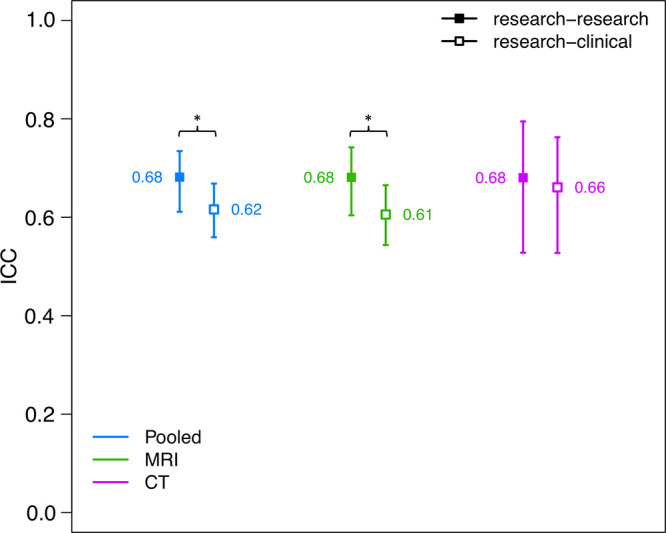
Background Various limitations have impacted research evaluating reader agreement for Liver Imaging Reporting and Data System (LI-RADS). Purpose To assess reader agreement of LI-RADS in an international multicenter multireader setting using scrollable images. Materials and Methods This retrospective study used deidentified clinical multiphase CT and MRI and reports with at least one untreated observation from six institutions and three countries; only qualifying examinations were submitted. Examination dates were October 2017 to August 2018 at the coordinating center. One untreated observation per examination was randomly selected using observation identifiers, and its clinically assigned features were extracted from the report. The corresponding LI-RADS version 2018 category was computed as a rescored clinical read. Each examination was randomly assigned to two of 43 research readers who independently scored the observation. Agreement for an ordinal modified four-category LI-RADS scale (LR-1, definitely benign; LR-2, probably benign; LR-3, intermediate probability of malignancy; LR-4, probably hepatocellular carcinoma [HCC]; LR-5, definitely HCC; LR-M, probably malignant but not HCC specific; and LR-TIV, tumor in vein) was computed using intraclass correlation coefficients (ICCs). Agreement was also computed for dichotomized malignancy (LR-4, LR-5, LR-M, and LR-TIV), LR-5, and LR-M. Agreement was compared between research-versus-research reads and research-versus-clinical reads. Results The study population consisted of 484 patients (mean age, 62 years ± 10 [SD]; 156 women; 93 CT examinations, 391 MRI examinations). ICCs for ordinal LI-RADS, dichotomized malignancy, LR-5, and LR-M were 0.68 (95% CI: 0.61, 0.73), 0.63 (95% CI: 0.55, 0.70), 0.58 (95% CI: 0.50, 0.66), and 0.46 (95% CI: 0.31, 0.61) respectively. Research-versus-research reader agreement was higher than research-versus-clinical agreement for modified four-category LI-RADS (ICC, 0.68 vs 0.62, respectively; P = .03) and for dichotomized malignancy (ICC, 0.63 vs 0.53, respectively; P = .005), but not for LR-5 (P = .14) or LR-M (P = .94). Conclusion There was moderate agreement for LI-RADS version 2018 overall. For some comparisons, research-versus-research reader agreement was higher than research-versus-clinical reader agreement, indicating differences between the clinical and research environments that warrant further study. © RSNA, 2023 Supplemental material is available for this article. See also the editorials by Johnson and Galgano and Smith in this issue.
Conflict of interest statement
Figures
![MRI scans show (A) reader disagreement and (B) reader agreement. (A)
Gadoxetic acid–enhanced MRI scans in a 56-year-old male patient with
cirrhosis secondary to hepatitis C. From left to right: contrast-unenhanced
(Pre), arterial phase (AP), portal venous phase (PVP), and hepatobiliary
phase (HBP) images. This 21-mm hepatobiliary phase hypointense observation
(arrow) was characterized on the clinical read as having nonrim arterial
phase hyperenhancement and washout appearance and was categorized as Liver
Imaging Reporting and Data System (LI-RADS) category LR-5 (definitely
hepatocellular carcinoma [HCC]). The first research reader characterized it
as having a targetoid appearance and categorized it as LR-M (probably or
definitely malignant, not specific for HCC). The second research reader
characterized it as having no major features and paralleling the blood pool
and categorized it as LR-2 (probably benign). It was subsequently resected
and found to be a well-differentiated HCC. (B) Extracellular
contrast–enhanced MRI scans in a 61-year-old female patient with
cirrhosis secondary to hepatitis C. From left to right: contrast-unenhanced,
arterial phase, portal venous phase, and delayed-phase (DP) images. This
31-mm observation (arrow) in the caudate lobe was characterized on the
clinical read as having arterial phase hyperenhancement, washout appearance,
and capsule appearance, and was categorized as LI-RADS category LR-5
(definitely HCC). Both research readers also categorized this observation as
LR-5. The patient died of intracranial hemorrhage a few months
later.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/70dc/10315518/9d8029290ef8/radiol.222855.fig3.jpg)
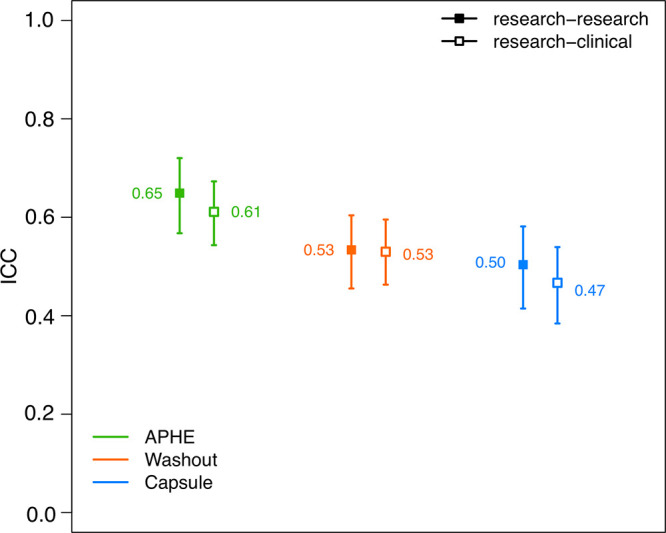
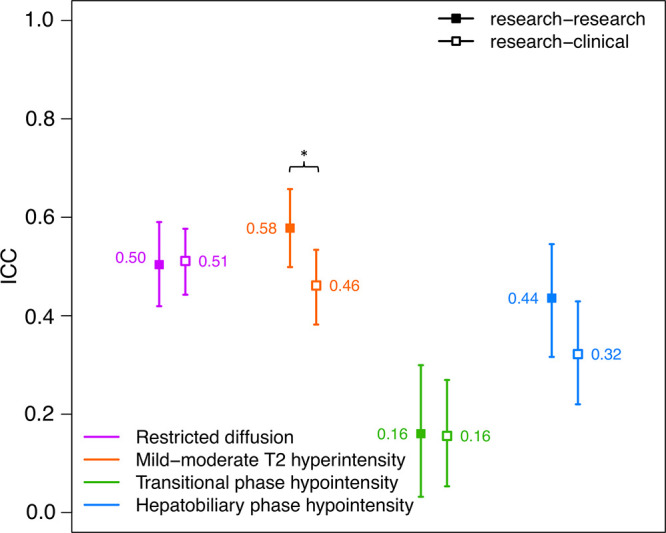
![Plot shows intraclass correlation coefficient (ICC) reader agreement
for dichotomized classification of Liver Imaging Reporting and Data System
(LI-RADS) version 2018 for the following dichotomized categories: probably
or definitely malignant versus other, LR-5 (definitely hepatocellular
carcinoma [HCC]) versus other, and LR-M (probably or definitely malignant,
not specific for HCC) versus other. Agreement among research reads only
(research-research; ■) and between research and clinical reads
(research-clinical; □) are shown. Tails represent 95% CIs. * P
< .05 by nonparametric bootstrap with per-case resampling.
Research-research agreement for malignant categories was better than
research-clinical agreement.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/70dc/10315518/9e221d726a19/radiol.222855.fig4.jpg)
Comment in
-
LI-RADS Version 2018 for MRI and CT: Interreader Agreement in Real-World Practice.Radiology. 2023 Jun;307(5):e231212. doi: 10.1148/radiol.231212. Radiology. 2023. PMID: 37367438 No abstract available.
-
Reliability of LI-RADS for MRI and CT: Is Excellence Achievable?Radiology. 2023 Jun;307(5):e231066. doi: 10.1148/radiol.231066. Radiology. 2023. PMID: 37367440 No abstract available.
References
-
- Chen N , Motosugi U , Morisaka H , et al . Added Value of a Gadoxetic Acid-enhanced Hepatocyte-phase Image to the LI-RADS System for Diagnosing Hepatocellular Carcinoma . Magn Reson Med Sci 2016. ; 15 ( 1 ): 49 – 59 . - PubMed
-
- Choi SH , Byun JH , Kim SY , et al . Liver Imaging Reporting and Data System v2014 With Gadoxetate Disodium-Enhanced Magnetic Resonance Imaging: Validation of LI-RADS Category 4 and 5 Criteria . Invest Radiol 2016. ; 51 ( 8 ): 483 – 490 . - PubMed
