

Dual Antiplatelet Therapy vs Alteplase for Patients With Minor Nondisabling Acute Ischemic Stroke: The ARAMIS Randomized Clinical Trial
- PMID: 37367978
- PMCID: PMC10300686
- DOI: 10.1001/jama.2023.7827
Dual Antiplatelet Therapy vs Alteplase for Patients With Minor Nondisabling Acute Ischemic Stroke: The ARAMIS Randomized Clinical Trial
Abstract
Importance: Intravenous thrombolysis is increasingly used in patients with minor stroke, but its benefit in patients with minor nondisabling stroke is unknown.
Objective: To investigate whether dual antiplatelet therapy (DAPT) is noninferior to intravenous thrombolysis among patients with minor nondisabling acute ischemic stroke.
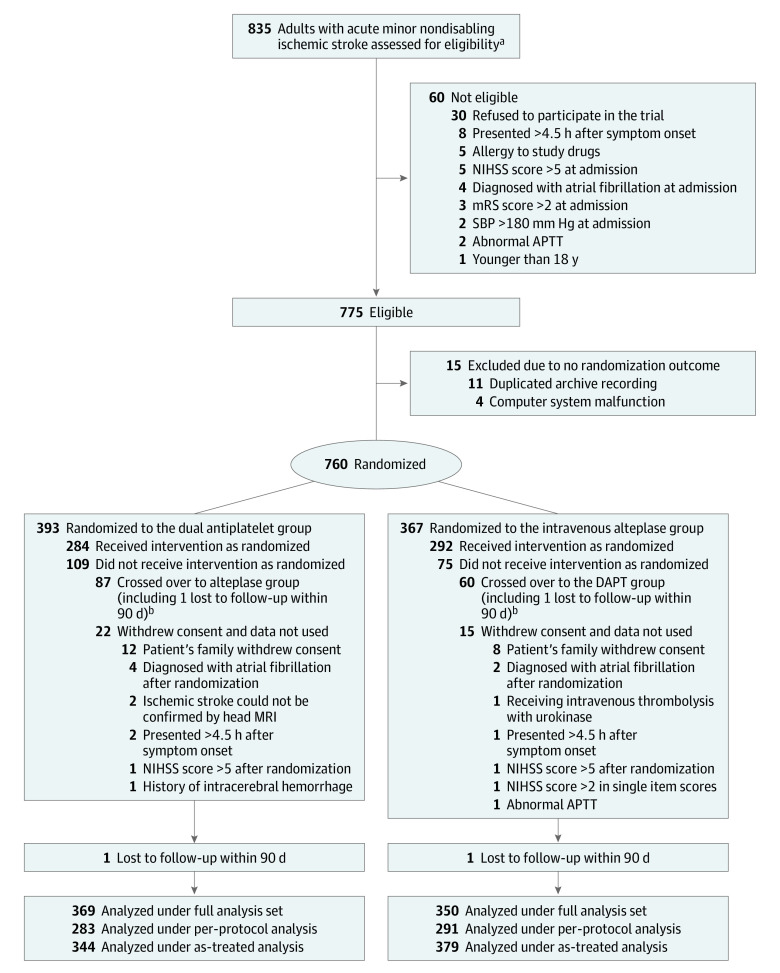
Design, setting, and participants: This multicenter, open-label, blinded end point, noninferiority randomized clinical trial included 760 patients with acute minor nondisabling stroke (National Institutes of Health Stroke Scale [NIHSS] score ≤5, with ≤1 point on the NIHSS in several key single-item scores; scale range, 0-42). The trial was conducted at 38 hospitals in China from October 2018 through April 2022. The final follow-up was on July 18, 2022.
Interventions: Eligible patients were randomized within 4.5 hours of symptom onset to the DAPT group (n = 393), who received 300 mg of clopidogrel on the first day followed by 75 mg daily for 12 (±2) days, 100 mg of aspirin on the first day followed by 100 mg daily for 12 (±2) days, and guideline-based antiplatelet treatment until 90 days, or the alteplase group (n = 367), who received intravenous alteplase (0.9 mg/kg; maximum dose, 90 mg) followed by guideline-based antiplatelet treatment beginning 24 hours after receipt of alteplase.
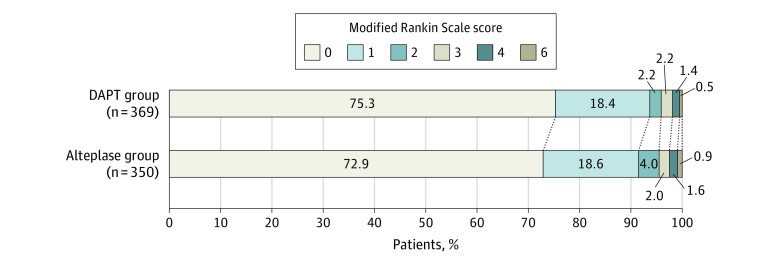
Main outcomes and measures: The primary end point was excellent functional outcome, defined as a modified Rankin Scale score of 0 or 1 (range, 0-6), at 90 days. The noninferiority of DAPT to alteplase was defined on the basis of a lower boundary of the 1-sided 97.5% CI of the risk difference greater than or equal to -4.5% (noninferiority margin) based on a full analysis set, which included all randomized participants with at least 1 efficacy evaluation, regardless of treatment group. The 90-day end points were assessed in a blinded manner. A safety end point was symptomatic intracerebral hemorrhage up to 90 days.
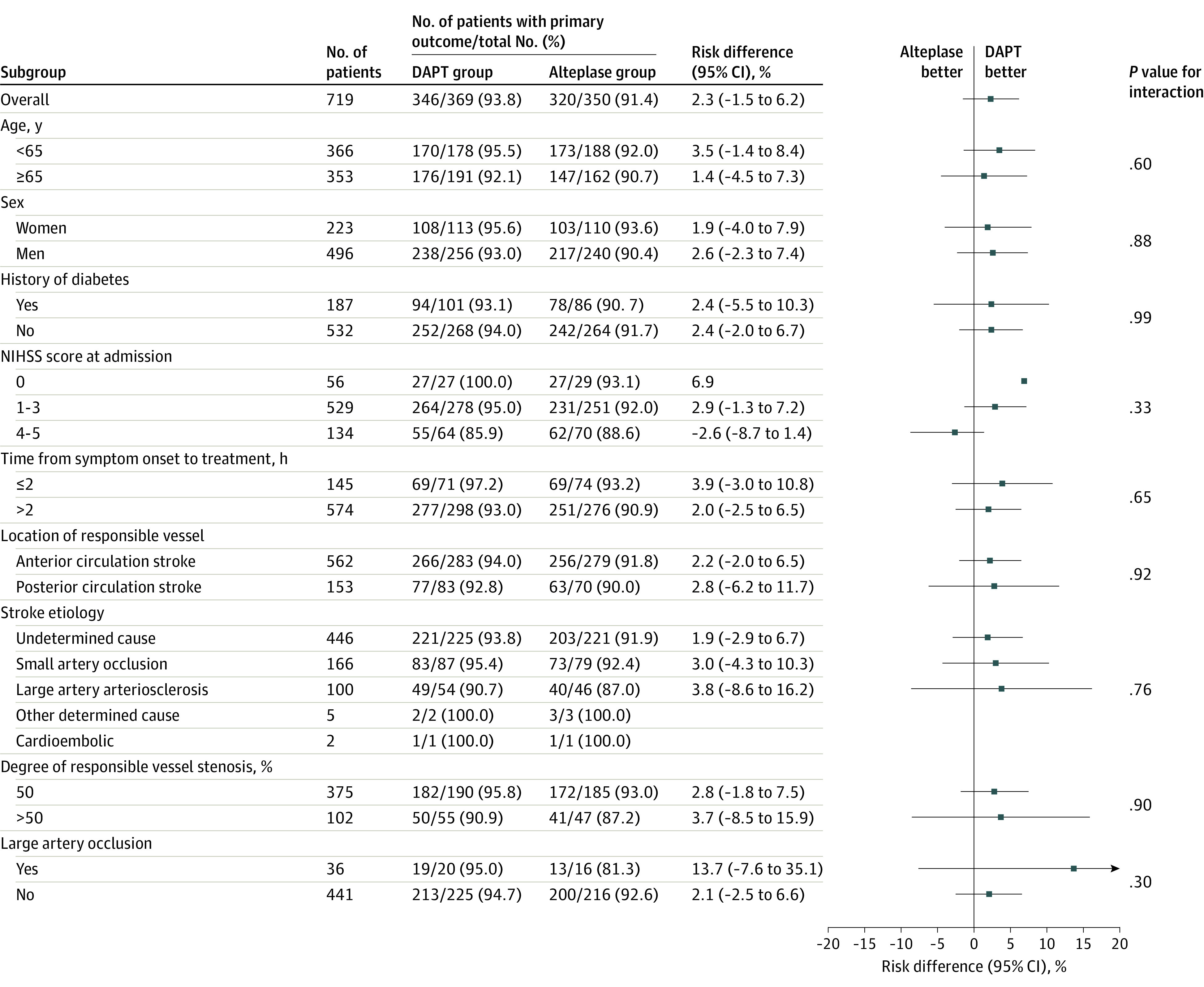
Results: Among 760 eligible randomized patients (median [IQR] age, 64 [57-71] years; 223 [31.0%] women; median [IQR] NIHSS score, 2 [1-3]), 719 (94.6%) completed the trial. At 90 days, 93.8% of patients (346/369) in the DAPT group and 91.4% (320/350) in the alteplase group had an excellent functional outcome (risk difference, 2.3% [95% CI, -1.5% to 6.2%]; crude relative risk, 1.38 [95% CI, 0.81-2.32]). The unadjusted lower limit of the 1-sided 97.5% CI was -1.5%, which is larger than the -4.5% noninferiority margin (P for noninferiority <.001). Symptomatic intracerebral hemorrhage at 90 days occurred in 1 of 371 participants (0.3%) in the DAPT group and 3 of 351 (0.9%) in the alteplase group.
Conclusions and relevance: Among patients with minor nondisabling acute ischemic stroke presenting within 4.5 hours of symptom onset, DAPT was noninferior to intravenous alteplase with regard to excellent functional outcome at 90 days.
Trial registration: ClinicalTrials.gov Identifier: NCT03661411.
Conflict of interest statement
Figures
Comment in
-
In minor, nondisabling, acute ischemic stroke, DAPT was noninferior to IV alteplase for excellent functional outcome at 90 d.Ann Intern Med. 2023 Oct;176(10):JC110. doi: 10.7326/J23-0072. Epub 2023 Oct 3. Ann Intern Med. 2023. PMID: 37782921
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi: 10.1161/STR.0000000000000211 - DOI - PubMed
-
- Liu L, Chen W, Zhou H, et al. ; Chinese Stroke Association Stroke Council Guideline Writing Committee . Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc Neurol. 2020;5(2):159-176. doi: 10.1136/svn-2020-000378 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
