

Using patient-derived tumor organoids from common epithelial cancers to analyze personalized T-cell responses to neoantigens
- PMID: 37368077
- PMCID: PMC10491521
- DOI: 10.1007/s00262-023-03476-6
Using patient-derived tumor organoids from common epithelial cancers to analyze personalized T-cell responses to neoantigens
Abstract
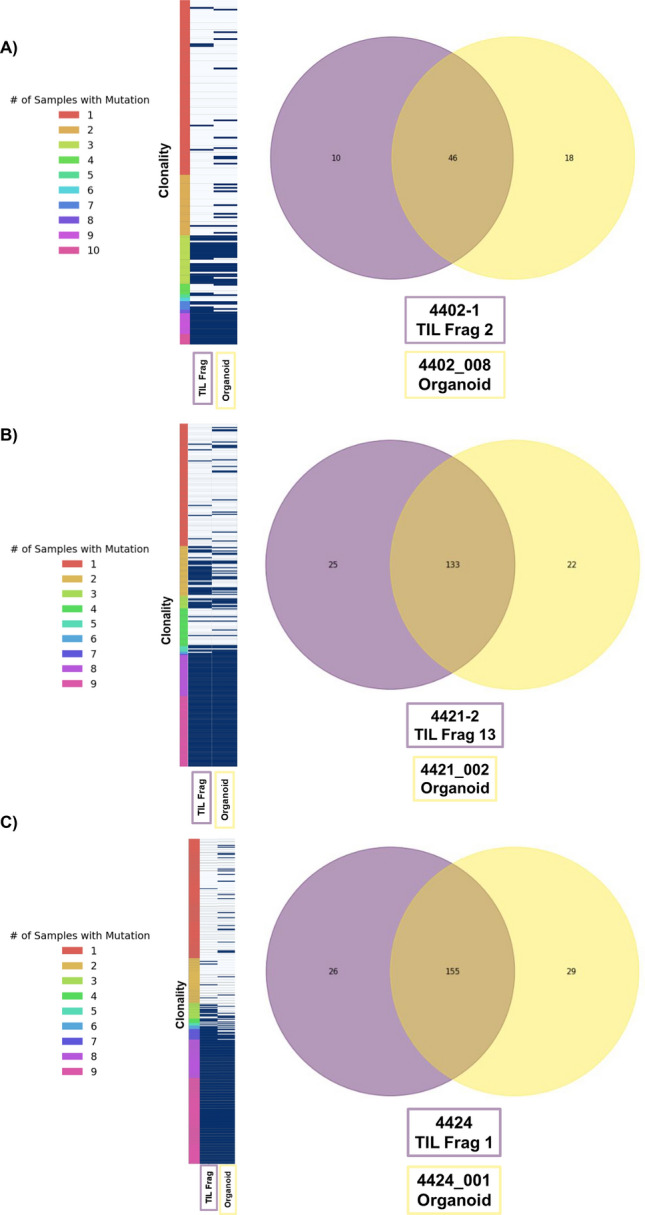
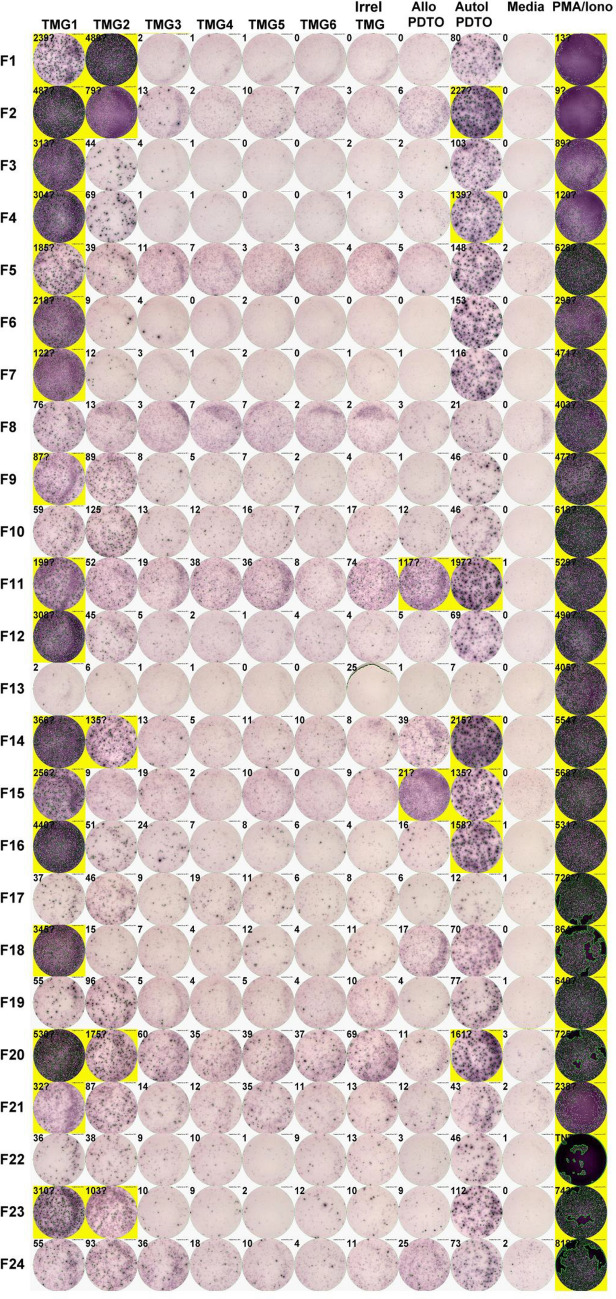
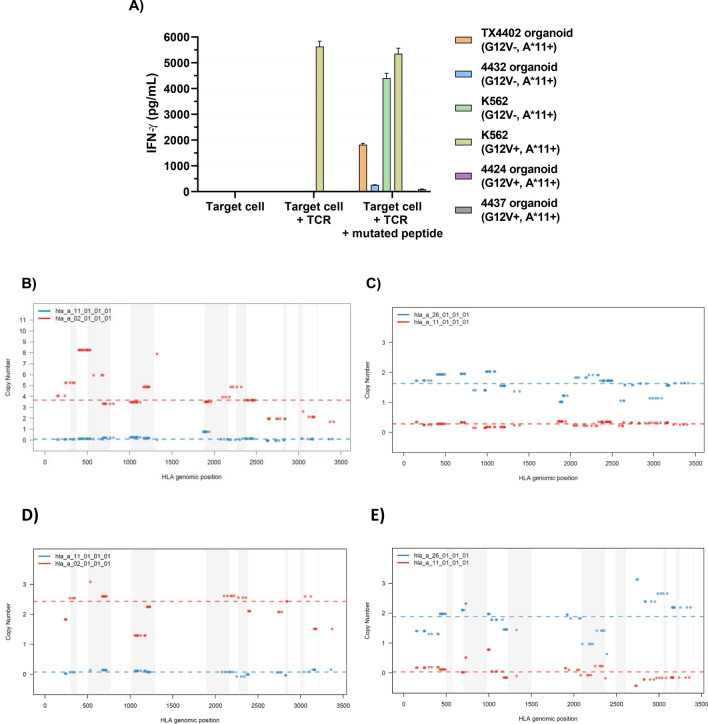
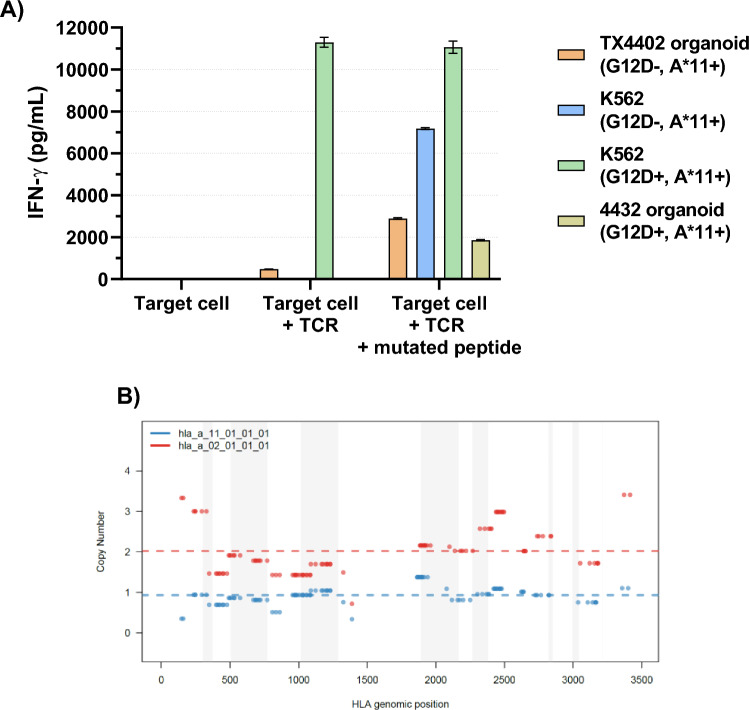
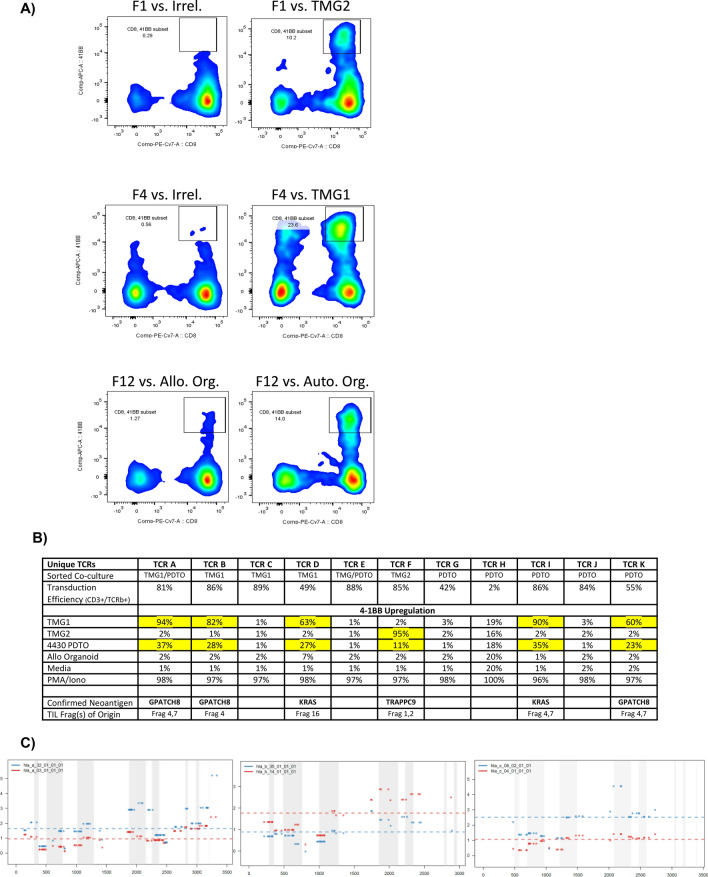
Adoptive cell transfer of tumor-infiltrating lymphocytes (TIL) can mediate durable complete responses in some patients with common epithelial cancers but does so infrequently. A better understanding of T-cell responses to neoantigens and tumor-related immune evasion mechanisms requires having the autologous tumor as a reagent. We investigated the ability of patient-derived tumor organoids (PDTO) to fulfill this need and evaluated their utility as a tool for selecting T-cells for adoptive cell therapy. PDTO established from metastases from patients with colorectal, breast, pancreatic, bile duct, esophageal, lung, and kidney cancers underwent whole exomic sequencing (WES), to define mutations. Organoids were then evaluated for recognition by autologous TIL or T-cells transduced with cloned T-cell receptors recognizing defined neoantigens. PDTO were also used to identify and clone TCRs from TIL targeting private neoantigens and define those tumor-specific targets. PDTO were successfully established in 38/47 attempts. 75% were available within 2 months, a timeframe compatible with screening TIL for clinical administration. These lines exhibited good genetic fidelity with their parental tumors, especially for mutations with higher clonality. Immunologic recognition assays demonstrated instances of HLA allelic loss not found by pan-HLA immunohistochemistry and in some cases WES of fresh tumor. PDTO could also be used to show differences between TCRs recognizing the same antigen and to find and clone TCRs recognizing private neoantigens. PDTO can detect tumor-specific defects blocking T-cell recognition and may have a role as a selection tool for TCRs and TIL used in adoptive cell therapy.
Keywords: Adoptive cell therapy; HLA loss-of-heterozygosity; Immune evasion; Immunotherapy; Organoids; Tumor-derived organoids.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
