

Real-world efficacy and safety of TACE plus camrelizumab and apatinib in patients with HCC (CHANCE2211): a propensity score matching study
- PMID: 37368105
- PMCID: PMC10667391
- DOI: 10.1007/s00330-023-09754-2
Real-world efficacy and safety of TACE plus camrelizumab and apatinib in patients with HCC (CHANCE2211): a propensity score matching study
Abstract
Objectives: This study aimed to investigate the efficacy and safety of transarterial chemoembolization (TACE) plus camrelizumab, a monoclonal antibody targeting programmed death-1, and apatinib for patients with intermediate and advanced hepatocellular carcinoma (HCC) in a real-world setting.
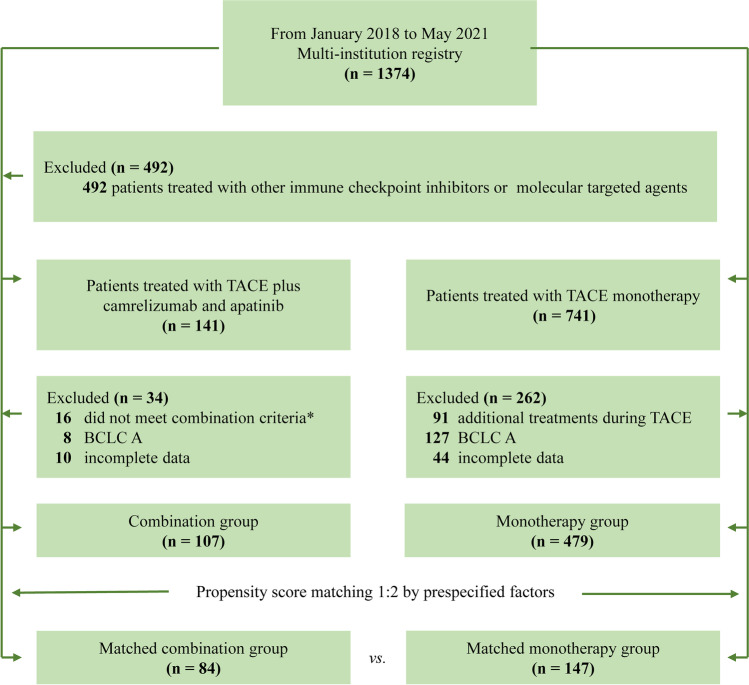
Methods: A total of 586 HCC patients treated with either TACE plus camrelizumab and apatinib (combination group, n = 107) or TACE monotherapy (monotherapy group, n = 479) were included retrospectively. Propensity score matching analysis was used to match patients. The overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and safety in the combination group were described in comparison to monotherapy.
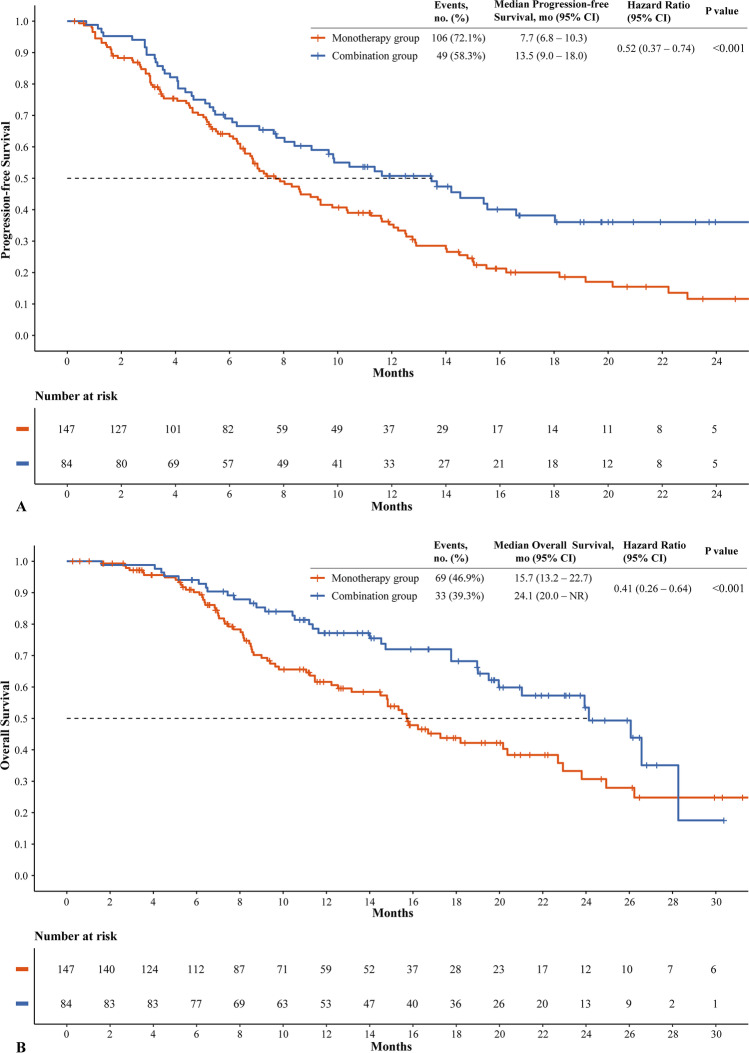
Results: After propensity score matching (1:2), 84 patients in the combination group were matched to 147 patients in the monotherapy group. The median age was 57 years and 71/84 (84.5%) patients were male in the combination group, while the median age was 57 years with 127/147 (86.4%) male in the monotherapy group. The median OS, PFS, and ORR in the combination group were significantly higher than those in the monotherapy group (median OS, 24.1 vs. 15.7 months, p = 0.008; median PFS, 13.5 vs. 7.7 months, p = 0.003; ORR, 59.5% [50/84] vs. 37.4% [55/147], p = 0.002). On multivariable Cox regression, combination therapy was associated with significantly better OS (adjusted hazard ratio [HR], 0.41; 95% confidence interval [CI], 0.26-0.64; p < 0.001) and PFS (adjusted HR, 0.52; 95% CI, 0.37-0.74; p < 0.001). Grade 3 or 4 adverse events occurred in 14/84 (16.7%) and 12/147 (8.2%) in the combination and monotherapy groups, respectively.
Conclusions: TACE plus camrelizumab and apatinib showed significantly better OS, PFS, and ORR versus TACE monotherapy for predominantly advanced HCC.
Clinical relevance statement: Compared with TACE monotherapy, TACE plus immunotherapy and molecular targeted therapy showed better clinical efficacy for predominantly advanced HCC patients, with a higher incidence of adverse events.
Key points: • This propensity score-matched study demonstrates that TACE plus immunotherapy and molecular targeted therapy have a longer OS, PFS, and ORR compared with TACE monotherapy in HCC. • Grade 3 or 4 adverse events occurred in 14/84 (16.7%) patients treated with TACE plus immunotherapy and molecular targeted therapy compared with 12/147 (8.2%) patients in the monotherapy group, while no grade 5 adverse events were observed in all cohorts.
Keywords: Carcinoma, hepatocellular; Chemoembolization, therapeutic; Combined modality therapy; Immunotherapy; Molecular targeted therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

References
-
- Sung H, Ferlay J, Siegel RL et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249 - PubMed
-
- Llovet JM, Kelley RK, Villanueva A et al (2021) Hepatocellular carcinoma. Nat Rev Dis Primers 7:6 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
