

Guideline Concordance of Treatment and Outcomes Among Adult Non-Hodgkin Lymphoma Patients in Sub-Saharan Africa: A Multinational, Population-Based Cohort
- PMID: 37368350
- PMCID: PMC10628567
- DOI: 10.1093/oncolo/oyad157
Guideline Concordance of Treatment and Outcomes Among Adult Non-Hodgkin Lymphoma Patients in Sub-Saharan Africa: A Multinational, Population-Based Cohort
Abstract
Background: Although non-Hodgkin lymphoma (NHL) is the 6th most common malignancy in Sub-Saharan Africa (SSA), little is known about its management and outcome. Herein, we examined treatment patterns and survival among NHL patients.
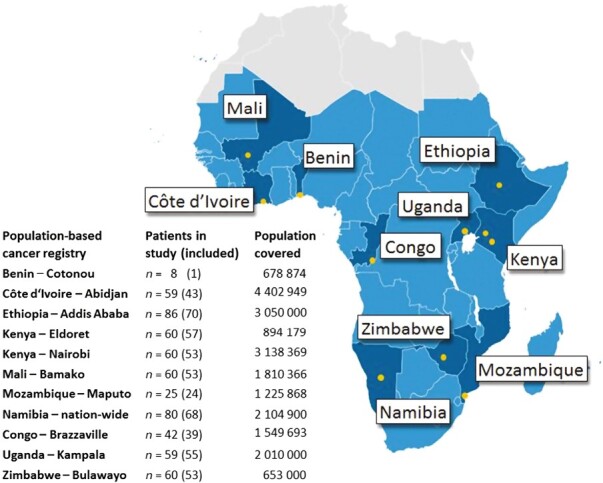
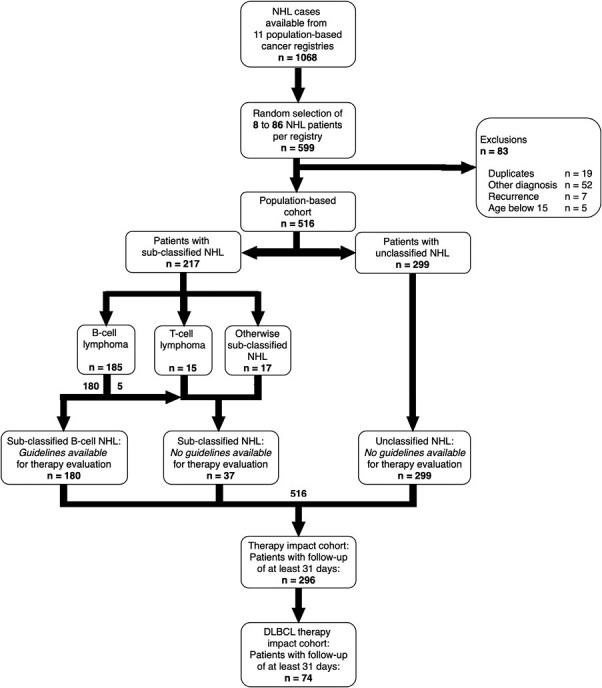
Methods: We obtained a random sample of adult patients diagnosed between 2011 and 2015 from 11 population-based cancer registries in 10 SSA countries. Descriptive statistics for lymphoma-directed therapy (LDT) and degree of concordance with National Comprehensive Cancer Network (NCCN) guidelines were calculated, and survival rates were estimated.
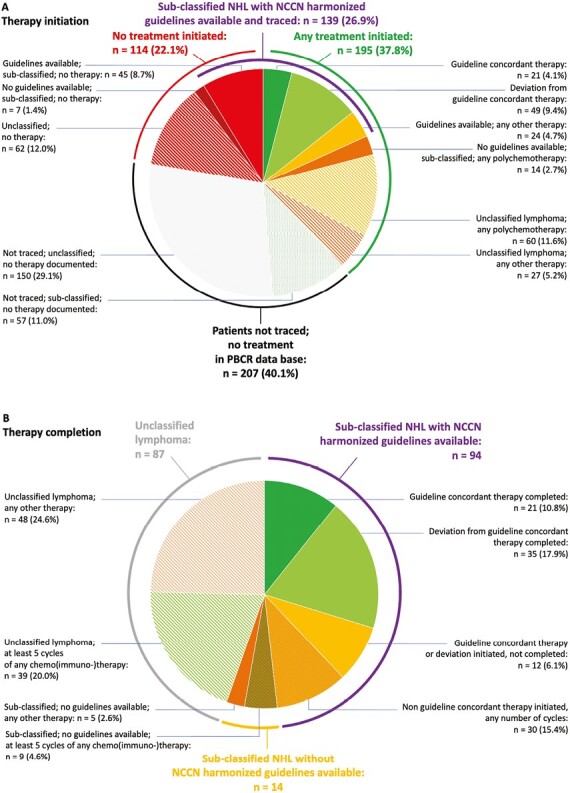
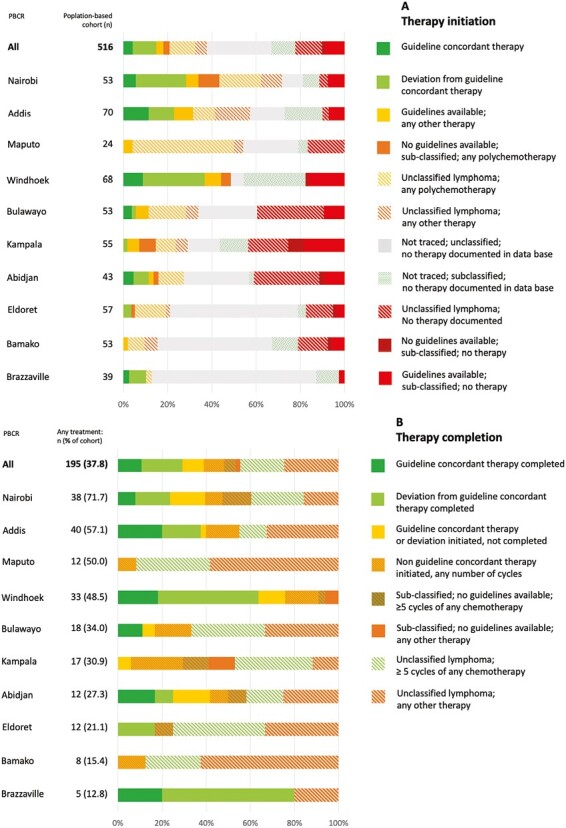
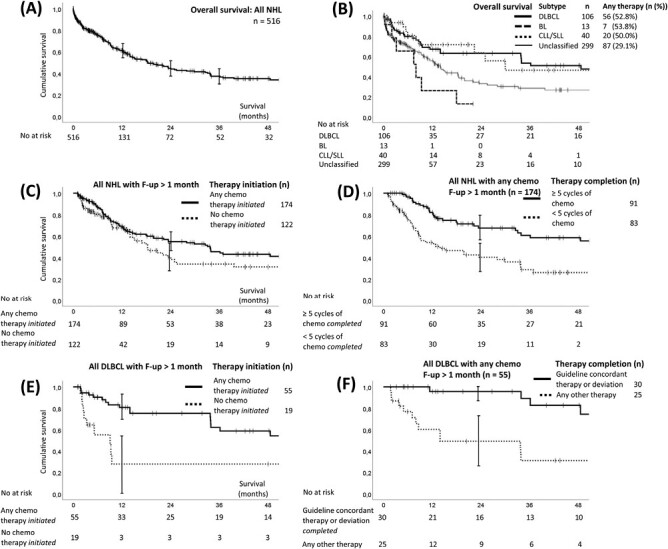
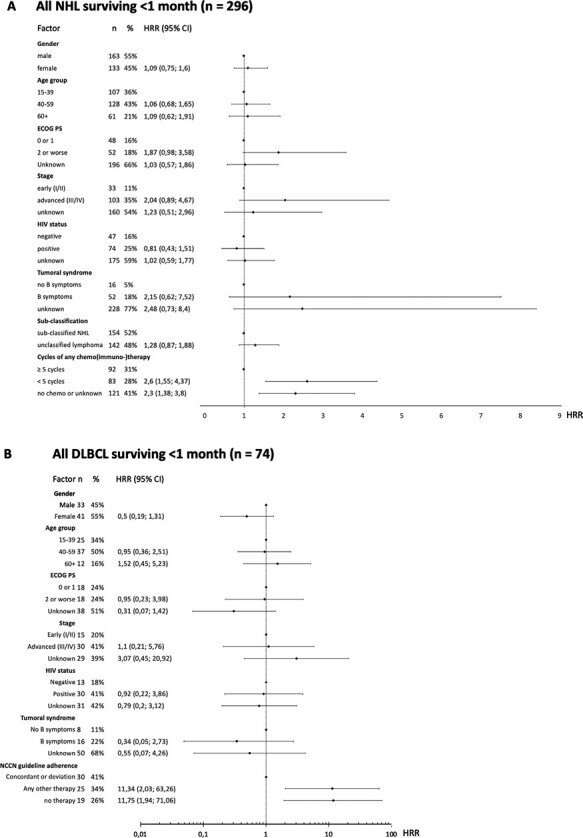
Findings: Of 516 patients included in the study, sub-classification was available for 42.1% (121 high-grade and 64 low-grade B-cell lymphoma, 15 T-cell lymphoma and 17 otherwise sub-classified NHL), whilst the remaining 57.9% were unclassified. Any LDT was identified for 195 of all patients (37.8%). NCCN guideline-recommended treatment was initiated in 21 patients. This corresponds to 4.1% of all 516 patients, and to 11.7% of 180 patients with sub-classified B-cell lymphoma and NCCN guidelines available. Deviations from guideline-recommended treatment were initiated in another 49 (9.5% of 516, 27.2% of 180). By registry, the proportion of all patients receiving guideline-concordant LDT ranged from 30.8% in Namibia to 0% in Maputo and Bamako. Concordance with treatment recommendations was not assessable in 75.1% of patients (records not traced (43.2%), traced but no sub-classification identified (27.8%), traced but no guidelines available (4.1%)). By registry, diagnostic work-up was in part importantly limited, thus impeding guideline evaluation significantly. Overall 1-year survival was 61.2% (95%CI 55.3%-67.1%). Poor ECOG performance status, advanced stage, less than 5 cycles and absence of chemo (immuno-) therapy were associated with unfavorable survival, while HIV status, age, and gender did not impact survival. In diffuse large B-cell lymphoma, initiation of guideline-concordant treatment was associated with favorable survival.
Interpretation: This study shows that a majority of NHL patients in SSA are untreated or undertreated, resulting in unfavorable survival. Investments in enhanced diagnostic services, provision of chemo(immuno-)therapy and supportive care will likely improve outcomes in the region.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
The authors indicated no conflict of interest.
Figures
References
-
- Mafra A, Laversanne M, Gospodarowicz M, et al. Global patterns of non-Hodgkin lymphoma in 2020. Int J Cancer. 2022;151(9):1474-1481. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
