

Contribution of Frailty to Multimorbidity Patterns and Trajectories: Longitudinal Dynamic Cohort Study of Aging People
- PMID: 37368462
- PMCID: PMC10365626
- DOI: 10.2196/45848
Contribution of Frailty to Multimorbidity Patterns and Trajectories: Longitudinal Dynamic Cohort Study of Aging People
Abstract
Background: Multimorbidity and frailty are characteristics of aging that need individualized evaluation, and there is a 2-way causal relationship between them. Thus, considering frailty in analyses of multimorbidity is important for tailoring social and health care to the specific needs of older people.
Objective: This study aimed to assess how the inclusion of frailty contributes to identifying and characterizing multimorbidity patterns in people aged 65 years or older.
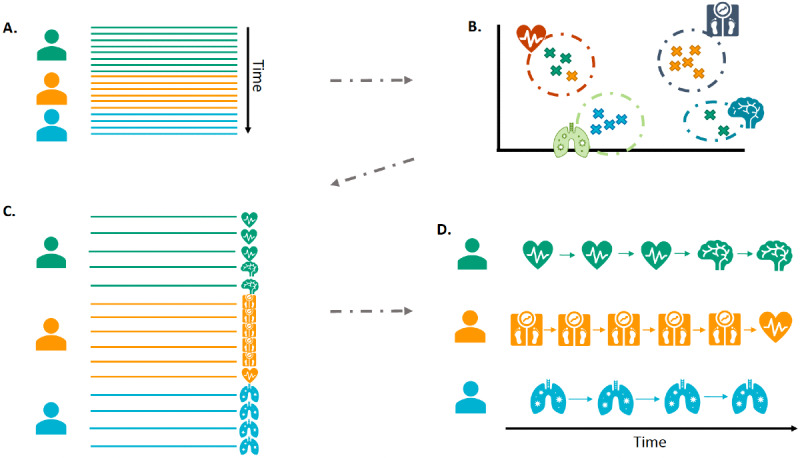
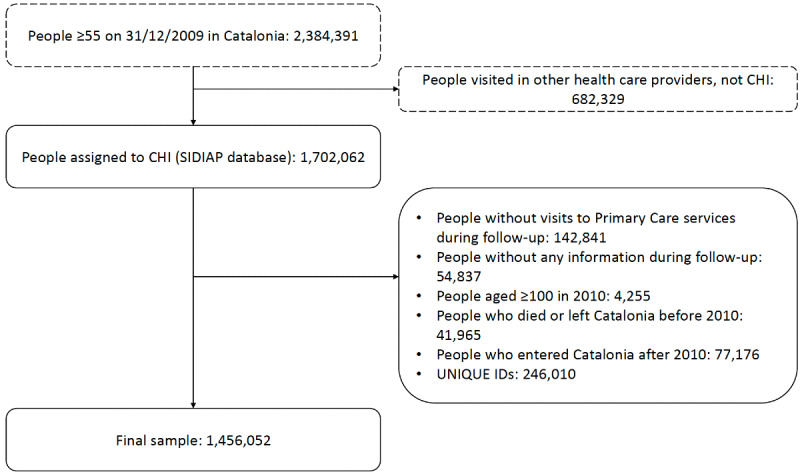
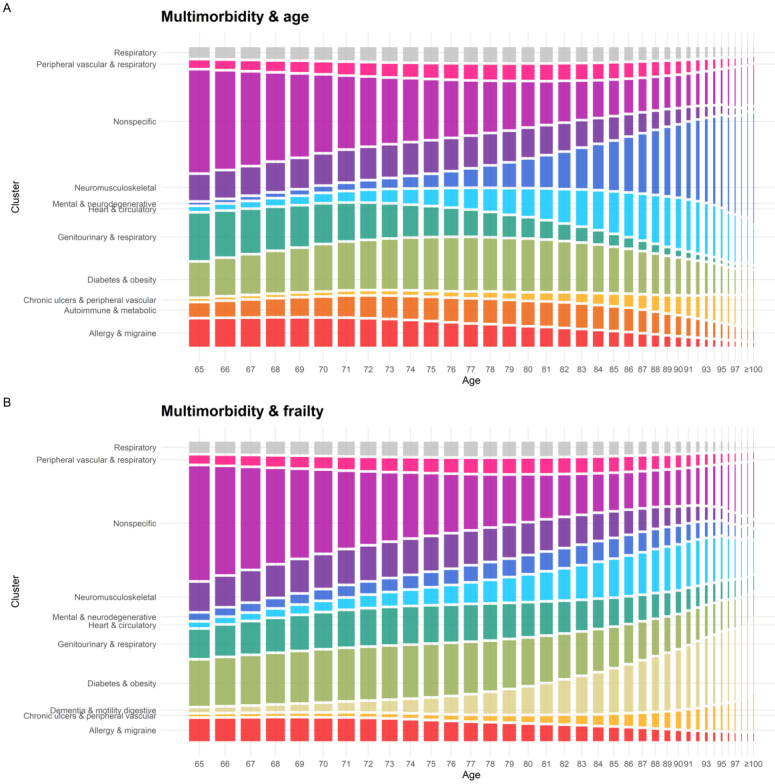
Methods: Longitudinal data were drawn from electronic health records through the SIDIAP (Sistema d'Informació pel Desenvolupament de la Investigació a l'Atenció Primària) primary care database for the population aged 65 years or older from 2010 to 2019 in Catalonia, Spain. Frailty and multimorbidity were measured annually using validated tools (eFRAGICAP, a cumulative deficit model; and Swedish National Study of Aging and Care in Kungsholmen [SNAC-K], respectively). Two sets of 11 multimorbidity patterns were obtained using fuzzy c-means. Both considered the chronic conditions of the participants. In addition, one set included age, and the other included frailty. Cox models were used to test their associations with death, nursing home admission, and home care need. Trajectories were defined as the evolution of the patterns over the follow-up period.
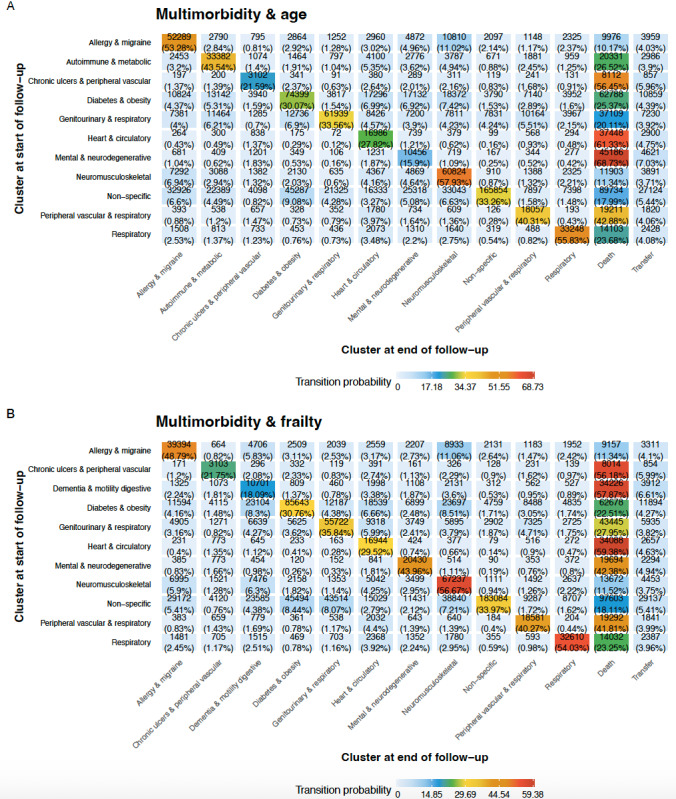
Results: The study included 1,456,052 unique participants (mean follow-up of 7.0 years). Most patterns were similar in both sets in terms of the most prevalent conditions. However, the patterns that considered frailty were better for identifying the population whose main conditions imposed limitations on daily life, with a higher prevalence of frail individuals in patterns like chronic ulcers &peripheral vascular. This set also included a dementia-specific pattern and showed a better fit with the risk of nursing home admission and home care need. On the other hand, the risk of death had a better fit with the set of patterns that did not include frailty. The change in patterns when considering frailty also led to a change in trajectories. On average, participants were in 1.8 patterns during their follow-up, while 45.1% (656,778/1,456,052) remained in the same pattern.
Conclusions: Our results suggest that frailty should be considered in addition to chronic diseases when studying multimorbidity patterns in older adults. Multimorbidity patterns and trajectories can help to identify patients with specific needs. The patterns that considered frailty were better for identifying the risk of certain age-related outcomes, such as nursing home admission or home care need, while those considering age were better for identifying the risk of death. Clinical and social intervention guidelines and resource planning can be tailored based on the prevalence of these patterns and trajectories.
Keywords: clustering; electronic health record; frailty; multimorbidity; primary care; trajectory.
©Lucía A Carrasco-Ribelles, Margarita Cabrera-Bean, Marc Danés-Castells, Edurne Zabaleta-del-Olmo, Albert Roso-Llorach, Concepción Violán. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org), 27.06.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people.EClinicalMedicine. 2022 Aug 11;52:101610. doi: 10.1016/j.eclinm.2022.101610. eCollection 2022 Oct. EClinicalMedicine. 2022. PMID: 36034409 Free PMC article.
-
Associations between multimorbidity and frailty transitions among older Americans.J Cachexia Sarcopenia Muscle. 2023 Apr;14(2):1075-1082. doi: 10.1002/jcsm.13197. Epub 2023 Feb 28. J Cachexia Sarcopenia Muscle. 2023. PMID: 36852679 Free PMC article.
-
Mortality, Falls, and Fracture Risk Are Positively Associated With Frailty: A SIDIAP Cohort Study of 890 000 Patients.J Gerontol A Biol Sci Med Sci. 2022 Jan 7;77(1):148-154. doi: 10.1093/gerona/glab102. J Gerontol A Biol Sci Med Sci. 2022. PMID: 33885746 Free PMC article.
-
Frailty and chronic disease.Panminerva Med. 2019 Dec;61(4):486-492. doi: 10.23736/S0031-0808.19.03731-5. Epub 2019 Jul 30. Panminerva Med. 2019. PMID: 31362483 Review.
-
Frailty and Multimorbidity: A Systematic Review and Meta-analysis.J Gerontol A Biol Sci Med Sci. 2019 Apr 23;74(5):659-666. doi: 10.1093/gerona/gly110. J Gerontol A Biol Sci Med Sci. 2019. PMID: 29726918
Cited by
-
Using electronic health records to understand multimorbidity in older people: a scoping review.Eur Geriatr Med. 2025 Aug;16(4):1163-1206. doi: 10.1007/s41999-025-01231-x. Epub 2025 Jul 3. Eur Geriatr Med. 2025. PMID: 40608251 Free PMC article. Review.
-
SARS-CoV-2 Infection Risk by Vaccine Doses and Prior Infections Over 24 Months: ProHEpiC-19 Longitudinal Study.JMIR Public Health Surveill. 2024 Nov 22;10:e56926. doi: 10.2196/56926. JMIR Public Health Surveill. 2024. PMID: 39648969 Free PMC article.
-
Polypharmacy and Potentially Inappropriate Medications in Adults ≥75 Years of Age by Dementia and Frailty Status: The ARIC Study.Mayo Clin Proc. 2025 May 17:S0025-6196(24)00667-0. doi: 10.1016/j.mayocp.2024.11.030. Online ahead of print. Mayo Clin Proc. 2025. PMID: 40380972
-
Investigating Frailty, Polypharmacy, Malnutrition, Chronic Conditions, and Quality of Life in Older Adults: Large Population-Based Study.JMIR Public Health Surveill. 2024 Oct 11;10:e50617. doi: 10.2196/50617. JMIR Public Health Surveill. 2024. PMID: 39145920 Free PMC article.
-
Charting the Pathways of Cardiometabolic Multimorbidity: A Systematic Review of Clinical Trajectories.J Clin Med. 2025 Apr 11;14(8):2615. doi: 10.3390/jcm14082615. J Clin Med. 2025. PMID: 40283445 Free PMC article. Review.
References
-
- Barnett K, Mercer S, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. The Lancet. 2012 Jul;380(9836):37–43. doi: 10.1016/s0140-6736(12)60240-2. doi: 10.1016/s0140-6736(12)60240-2. - DOI - DOI - PubMed
-
- Clegg A, Young J, Iliffe S, Rikkert M, Rockwood K. Frailty in elderly people. The Lancet. 2013 Mar;381(9868):752–762. doi: 10.1016/s0140-6736(12)62167-9. https://doi.org/10 - DOI - PMC - PubMed
-
- Rockwood K, Mitnitski A, Song X, Steen B, Skoog I. Long-term risks of death and institutionalization of elderly people in relation to deficit accumulation at age 70. J Am Geriatr Soc. 2006 Jun;54(6):975–9. doi: 10.1111/j.1532-5415.2006. doi: 10.1111/j.1532-5415.2006.00738.x.JGS738 - DOI - DOI - PubMed
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, Cardiovascular Health Study Collaborative Research Group Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001 Mar 01;56(3):M146–56. doi: 10.1093/gerona/56.3.m146. https://doi.org/10 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
