

Future targets for migraine treatment beyond CGRP
- PMID: 37370051
- PMCID: PMC10304392
- DOI: 10.1186/s10194-023-01567-4
Future targets for migraine treatment beyond CGRP
Abstract
Background: Migraine is a disabling and chronic neurovascular headache disorder. Trigeminal vascular activation and release of calcitonin gene-related peptide (CGRP) play a pivotal role in the pathogenesis of migraine. This knowledge has led to the development of CGRP(-receptor) therapies. Yet, a substantial proportion of patients do not respond to these treatments. Therefore, alternative targets for future therapies are warranted. The current narrative review provides a comprehensive overview of the pathophysiological role of these possible non-CGRP targets in migraine.
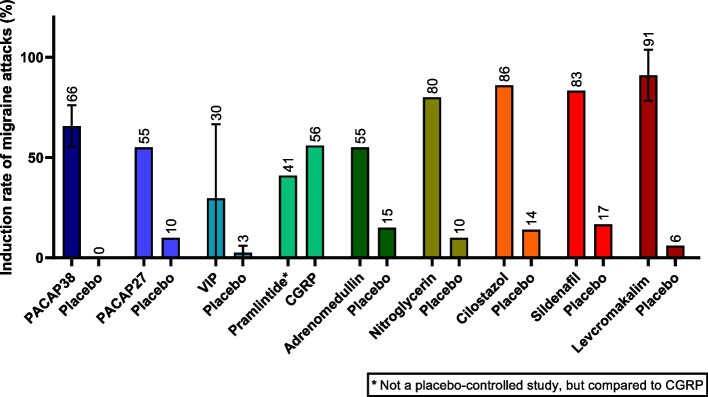
Findings: We covered targets of the metabotropic receptors (pituitary adenylate cyclase-activating polypeptide (PACAP), vasoactive intestinal peptide (VIP), amylin, and adrenomedullin), intracellular targets (nitric oxide (NO), phosphodiesterase-3 (PDE3) and -5 (PDE5)), and ion channels (potassium, calcium, transient receptor potential (TRP), and acid-sensing ion channels (ASIC)). The majority of non-CGRP targets were able to induce migraine-like attacks, except for (i) calcium channels, as it is not yet possible to directly target channels to elucidate their precise involvement in migraine; (ii) TRP channels, activation of which can induce non-migraine headache; and (iii) ASICs, as their potential in inducing migraine attacks has not been investigated thus far. Drugs that target its receptors exist for PACAP, NO, and the potassium, TRP, and ASIC channels. No selective drugs exist for the other targets, however, some existing (migraine) treatments appear to indirectly antagonize responses to amylin, adrenomedullin, and calcium channels. Drugs against PACAP, NO, potassium channels, TRP channels, and only a PAC1 antibody have been tested for migraine treatment, albeit with ambiguous results.
Conclusion: While current research on these non-CGRP drug targets has not yet led to the development of efficacious therapies, human provocation studies using these targets have provided valuable insight into underlying mechanisms of migraine headaches and auras. Further studies are needed on these alternative therapies in non-responders of CGRP(-receptor) targeted therapies with the ultimate aim to pave the way towards a headache-free future for all migraine patients.
Keywords: Adrenomedullin; Amylin; Ion channels; Migraine; Nitric oxide; Non-CGRP targets; Phosphodiesterases; Pituitary adenylate cyclase-activating polypeptide; Vasoactive intestinal polypeptide.
© 2023. The Author(s).
Conflict of interest statement
Linda Al-Hassany, Deirdre M. Boucherie, Hannah Creeney, Ruben W.A.van Drie, Fatemeh Farham, Silvia Favaretto, Grangeon Lou, Hannah Lyons, Karol Marschollek, Dilara Onan, Umberto Pensato, Emily Stanyer, Marta Waliszewska-Prosół, Hui Zhou Chen declare no conflict of interest. Cédric Gollion reports speaker fees from Teva, Novartis, Lundbeck and Lilly. Wietse Wiels declares to have received an FWO Vlaanderen Fundamental Research scholarship. Faisal Mohammad Amin has received Honoraria or personal fees from Pfizer, Teva, Novartis, Lundbeck and Eli Lilly for lecturing or participating in advisory boards; is principal investigator for phase IV trials sponsored by Novartis and by Teva; serves as president of Danish Headache Society and board member of the European Headache Federation; serves as associate editor for Acta Neurol Scand, Front Neurol, Front Res Pain, and Headache Medicine; serves as junior associate editor for Cephalalgia and Cephalalgia Reports; member of the editorial board of J Headache Pain.
Figures

References
-
- Headache Classification Committee of the International Headache Society (IHS) (2018) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38(1):1–211 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
