

Hemodynamic parameters in patients undergoing surgery for pheochromocytoma/paraganglioma: a retrospective study
- PMID: 37370080
- PMCID: PMC10294368
- DOI: 10.1186/s12957-023-03072-z
Hemodynamic parameters in patients undergoing surgery for pheochromocytoma/paraganglioma: a retrospective study
Erratum in
-
Correction: Hemodynamic parameters in patients undergoing surgery for pheochromocytoma/paraganglioma: a retrospective study.World J Surg Oncol. 2023 Sep 19;21(1):298. doi: 10.1186/s12957-023-03181-9. World J Surg Oncol. 2023. PMID: 37723531 Free PMC article. No abstract available.
Abstract
Background: Pheochromocytoma (PHEO) and paraganglioma (PGL) are rare neuroendocrine tumors characterized by hemodynamic instability, caused by the paroxysmal release of catecholamines. Patients may develop cardiovascular complications in the perioperative phase due to the massive release of catecholamines, particularly during anesthetic induction and surgical manipulation of the tumor. The aim of this retrospective study was to evaluate the risk factors involved in perioperative hemodynamic instability in patients who underwent surgery for chromaffin tumors.
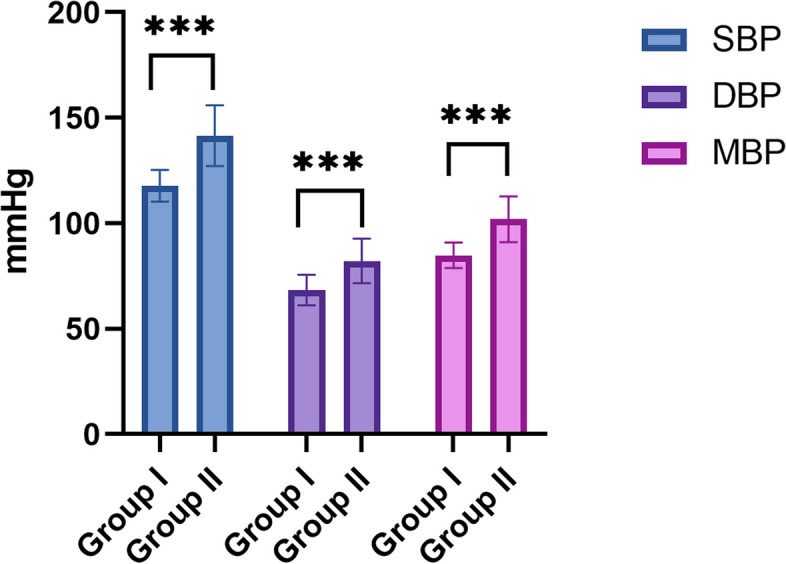
Methods: Forty patients (median age 55 [36.50-64.50]) undergone surgery for PHEO/abdominal PGL from January 2011 to December 2016 at the AOU Careggi (Florence, Italy) were retrospectively evaluated. Systolic, diastolic, and mean blood pressure were considered at baseline and during surgery. Patients with blood pressure steadily < 140/90 mmHg before surgery were considered "adequately prepared". A preoperative therapy with doxazosin, a selective alpha-1 blocker, was started in all patients for at least 14 days prior to the surgery. The presence of hemodynamic instability was reported.
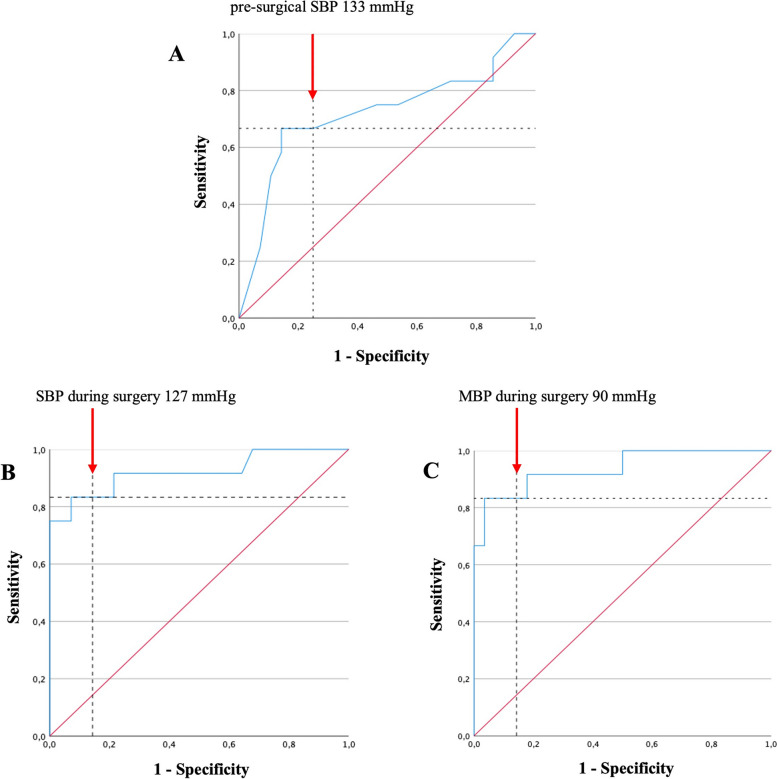
Results: Comparing males and females, a significant difference in doxazosin daily dose (p = 0.018), systolic blood pressure (p = 0.048), and in the proportion of adequately prepared patients (p = 0.031) emerged. A positive correlation between preoperative daily dose of doxazosin, tumor size (B = 0.60, p < 0.001), and urinary normetanephrine levels (B = 0.64, p < 0.001) was also observed. Hemodynamic instability occurred in 30.0% of patients. The absence of adequate preparation (p = 0.012) before surgery, urinary normetanephrine levels (NMNur p = 0.039), and surgery time (minutes) (p = 0.021) resulted as risk factors of hemodynamic instability in our series. The use of intraoperative drugs was higher in patients with hemodynamic instability (p < 0.001). A pre-surgical SBP level of > 133 mmHg (OR = 6 CI95% 1.37-26.20, p = 0.017) and an intraoperative SBP and MBP levels of > 127 mmHg (OR = 28.80 CI95% 2.23-371.0, p = 0.010) and > 90 mmHg (OR = 18.90 CI95% 1.82-196.0, p = 0.014), respectively, were identified as effective thresholds to recognize patients at higher risk of HI.
Conclusions: A preoperative therapy with alpha-blockers is useful, but not sufficient to avoid surgical risks. Patients with higher pre-surgical levels of NMNur, pre-surgical SBP > 133 mmHg, and/or intraoperative SBP > 127 mmHg and MBP > 90 mmHg, should be carefully monitored. A multidisciplinary approach is indispensable to optimize the management of PHEOs/abdominal PGLs in order to reduce surgical complications.
Keywords: Anesthesia; Endocrine; Oncology; Paraganglioma; Pheochromocytoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Chen H, Sippel RS, O'Dorisio MS, Vinik AI, Lloyd RV, Pacak K. The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas. 2010;39(6):775–783. doi: 10.1097/MPA.0b013e3181ebb4f0. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
