

What Imaging Modality Is More Effective in Predicting Early Recurrence of Hepatocellular Carcinoma after Hepatectomy Using Radiomics Analysis: CT or MRI or Both?
- PMID: 37370907
- PMCID: PMC10297510
- DOI: 10.3390/diagnostics13122012
What Imaging Modality Is More Effective in Predicting Early Recurrence of Hepatocellular Carcinoma after Hepatectomy Using Radiomics Analysis: CT or MRI or Both?
Abstract
Background: It is of great importance to predict the early recurrence (ER) of hepatocellular carcinoma (HCC) after hepatectomy using preoperative imaging modalities. Nevertheless, no comparative studies have been conducted to determine which modality, CT or MRI with radiomics analysis, is more effective.
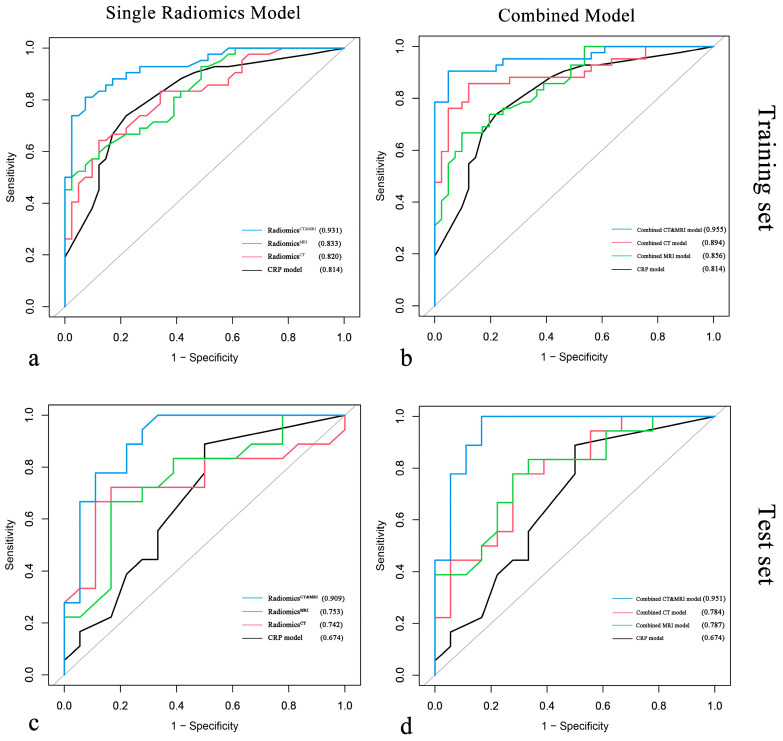
Methods: We retrospectively enrolled 119 HCC patients who underwent preoperative CT and MRI. A total of 3776 CT features and 4720 MRI features were extracted from the whole tumor. The minimum redundancy and maximum relevance algorithm (MRMR) and least absolute shrinkage and selection operator (LASSO) regression were applied for feature selection, then support vector machines (SVMs) were applied for model construction. Multivariable logistic regression analysis was employed to construct combined models that integrate clinical-radiological-pathological (CRP) traits and radscore. Receiver operating characteristic (ROC) curves, calibration curves, and decision curve analysis (DCA) were used to compare the efficacy of CT, MRI, and CT and MRI models in the test cohort.
Results: The CT model and MRI model showed no significant difference in the prediction of ER in HCC patients (p = 0.911). RadiomicsCT&MRI demonstrated a superior predictive performance than either RadiomicsCT or RadiomicsMRI alone (p = 0.032, 0.039). The combined CT and MRI model can significantly stratify patients at high risk of ER (area under the curve (AUC) of 0.951 in the training set and 0.955 in the test set) than the CT model (AUC of 0.894 and 0.784) and the MRI model (AUC of 0.856 and 0.787). DCA demonstrated that the CT and MRI model provided a greater net benefit than the models without radiomics analysis.
Conclusions: No significant difference was found in predicting the ER of HCC between CT models and MRI models. However, the multimodal radiomics model derived from CT and MRI can significantly improve the prediction of ER in HCC patients after resection.
Keywords: early recurrence; hepatocellular carcinoma; prediction; radiomics.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures





Similar articles
-
CT-based peritumoral radiomics signatures to predict early recurrence in hepatocellular carcinoma after curative tumor resection or ablation.Cancer Imaging. 2019 Feb 27;19(1):11. doi: 10.1186/s40644-019-0197-5. Cancer Imaging. 2019. PMID: 30813956 Free PMC article. Clinical Trial.
-
CT-Based Radiomics Nomogram Improves Risk Stratification and Prediction of Early Recurrence in Hepatocellular Carcinoma After Partial Hepatectomy.Front Oncol. 2022 Jul 7;12:896002. doi: 10.3389/fonc.2022.896002. eCollection 2022. Front Oncol. 2022. PMID: 35875140 Free PMC article.
-
Radiomics nomogram for prediction of glypican-3 positive hepatocellular carcinoma based on hepatobiliary phase imaging.Front Oncol. 2023 Sep 29;13:1209814. doi: 10.3389/fonc.2023.1209814. eCollection 2023. Front Oncol. 2023. PMID: 37841420 Free PMC article.
-
Radiomics for preoperative prediction of early recurrence in hepatocellular carcinoma: a meta-analysis.Front Oncol. 2023 Jun 7;13:1114983. doi: 10.3389/fonc.2023.1114983. eCollection 2023. Front Oncol. 2023. PMID: 37350952 Free PMC article.
-
Study Progress of Noninvasive Imaging and Radiomics for Decoding the Phenotypes and Recurrence Risk of Bladder Cancer.Front Oncol. 2021 Jul 15;11:704039. doi: 10.3389/fonc.2021.704039. eCollection 2021. Front Oncol. 2021. PMID: 34336691 Free PMC article. Review.
Cited by
-
Artificial intelligence in predicting recurrence after first-line treatment of liver cancer: a systematic review and meta-analysis.BMC Med Imaging. 2024 Oct 7;24(1):263. doi: 10.1186/s12880-024-01440-z. BMC Med Imaging. 2024. PMID: 39375586 Free PMC article.
References
-
- Akinyemiju T., Abera S., Ahmed M., Alam N., Alemayohu M.A., Allen C., Al-Raddadi R., Alvis-Guzman N., Amoako Y., Artaman A., et al. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3:1683–1691. doi: 10.1001/jamaoncol.2017.3055. - DOI - PMC - PubMed
-
- Dimitroulis D., Damaskos C., Valsami S., Davakis S., Garmpis N., Spartalis E., Athanasiou A., Moris D., Sakellariou S., Kykalos S., et al. From diagnosis to treatment of hepatocellular carcinoma: An epidemic problem for both developed and developing world. World J. Gastroenterol. 2017;23:5282–5294. doi: 10.3748/wjg.v23.i29.5282. - DOI - PMC - PubMed
-
- Liu Y.-W., Yong C.-C., Lin C.-C., Wang C.-C., Chen C.-L., Cheng Y.-F., Wang J.-H., Yen Y.-H. Six months as a cutoff time point to define early recurrence after liver resection of hepatocellular carcinoma based on post-recurrence survival. Updat. Surg. 2021;73:399–409. doi: 10.1007/s13304-020-00931-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
