

Aldosterone: Essential for Life but Damaging to the Vascular Endothelium
- PMID: 37371584
- PMCID: PMC10296074
- DOI: 10.3390/biom13061004
Aldosterone: Essential for Life but Damaging to the Vascular Endothelium
Abstract
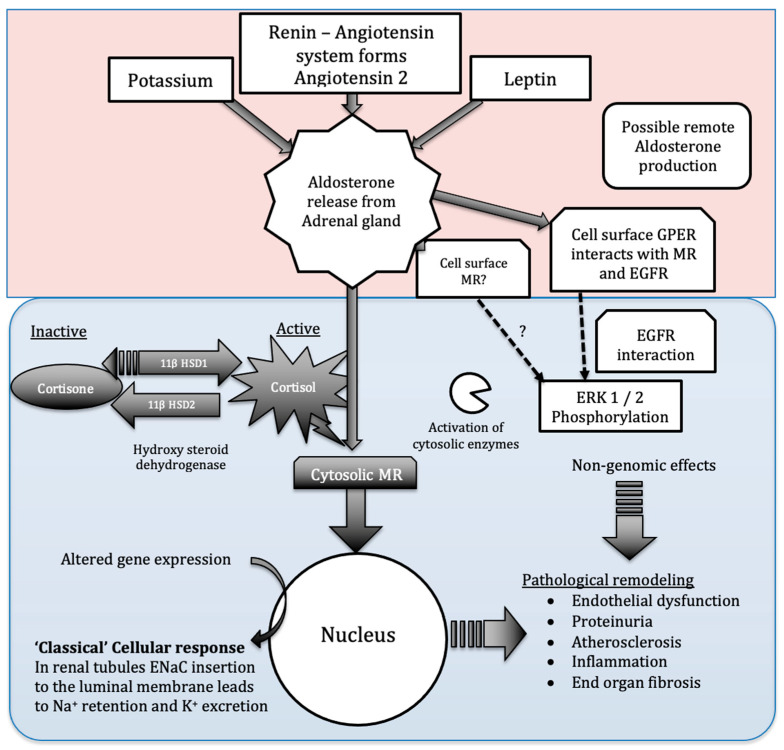
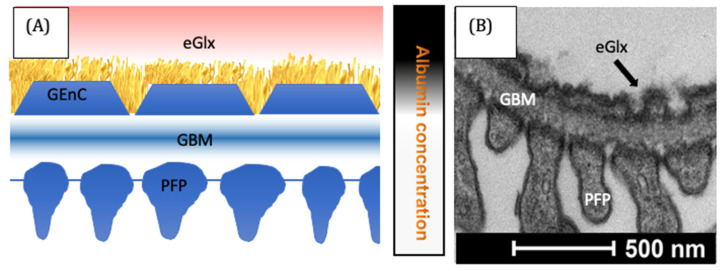
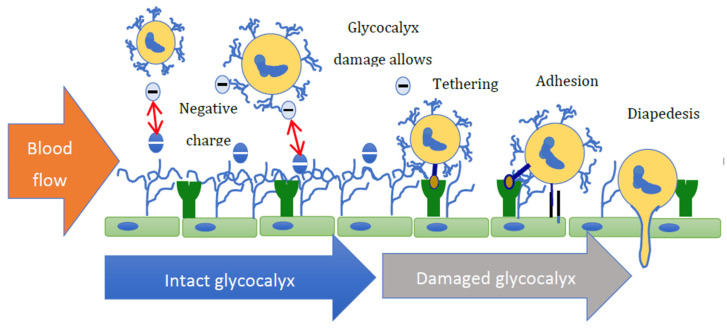
The renin angiotensin aldosterone system is a key regulator of blood pressure. Aldosterone is the final effector of this pathway, acting predominantly via mineralocorticoid receptors. Aldosterone facilitates the conservation of sodium and, with it, water and acts as a powerful stimulus for potassium excretion. However, evidence for the pathological impact of excess mineralocorticoid receptor stimulation is increasing. Here, we discussed how in the heart, hyperaldosteronism is associated with fibrosis, cardiac dysfunction, and maladaptive hypertrophy. In the kidney, aldosterone was shown to cause proteinuria and fibrosis and may contribute to the progression of kidney disease. More recently, studies suggested that aldosterone excess damaged endothelial cells. Here, we reviewed how damage to the endothelial glycocalyx may contribute to this process. The endothelial glycocalyx is a heterogenous, negatively charged layer on the luminal surface of cells. Aldosterone exposure alters this layer. The resulting structural changes reduced endothelial reactivity in response to protective shear stress, altered permeability, and increased immune cell trafficking. Finally, we reviewed current therapeutic strategies for limiting endothelial damage and suggested that preventing glycocalyx remodelling in response to aldosterone exposure may provide a novel strategy, free from the serious adverse effect of hyperkalaemia seen in response to mineralocorticoid blockade.
Keywords: aldosterone; endothelium; glycocalyx; mineralocorticoid receptor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gomez-Sanchez C., Holland O.B., Higgins J.R., Kem D.C., Kaplan N.M. Circadian rhythms of serum renin activity and serum corticosterone, prolactin, and aldosterone concentrations in the male rat on normal and low-sodium diets. Endocrinology. 1976;99:567–572. doi: 10.1210/endo-99-2-567. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- FS/CRTF/22/24361/BHF_/British Heart Foundation/United Kingdom
- MR/T031921/1/MRC_/Medical Research Council/United Kingdom
- PG/20/10187/BHF_/British Heart Foundation/United Kingdom
- MR/T031921/1/MRC/MRC_/Medical Research Council/United Kingdom
- MR/M018237/1/MRC/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
