

Current Therapies for Cholestatic Diseases
- PMID: 37371808
- PMCID: PMC10296345
- DOI: 10.3390/biomedicines11061713
Current Therapies for Cholestatic Diseases
Abstract
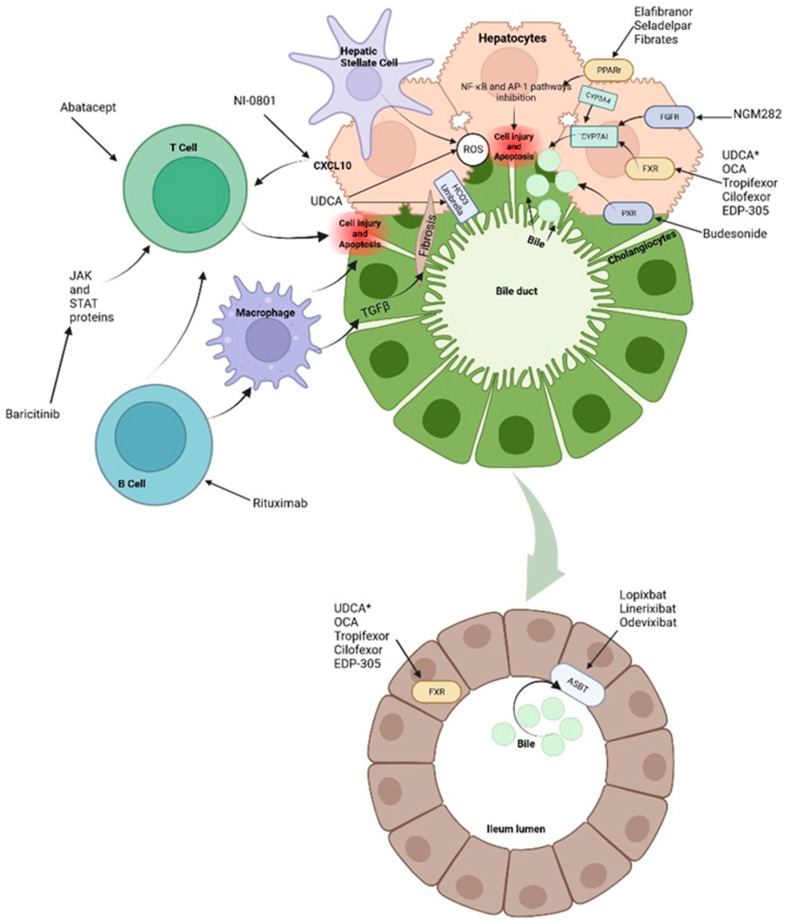
Cholestasis is a condition characterized by decrease in bile flow due to progressive pathological states that lead to chronic cholestatic liver diseases which affect the biliary tree at the intrahepatic level and extrahepatic level. They induce complications such as cirrhosis, liver failure, malignancies, bone disease and nutritional deficiencies that merit close follow-up and specific interventions. Furthermore, as those conditions progress to liver cirrhosis, there will be an increase in mortality but also an important impact in quality of life and economic burden due to comorbidities related with liver failure. Therefore, it is important that clinicians understand the treatment options for cholestatic liver diseases. With a general view of therapeutic options and their molecular targets, this review addresses the pathophysiology of cholangiopathies. The objective is to provide clinicians with an overview of the safety and efficacy of the treatment of cholangiopathies based on the current evidence.
Keywords: FXR agonist; PXR agonist; bile acids; cholestasis; fibreates; fibrosis; ursodeoxycholic acid.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
