

Molecular-Biology-Driven Frontline Treatment for Chronic Lymphocytic Leukemia: A Network Meta-Analysis of Randomized Clinical Trials
- PMID: 37373078
- PMCID: PMC10298034
- DOI: 10.3390/ijms24129930
Molecular-Biology-Driven Frontline Treatment for Chronic Lymphocytic Leukemia: A Network Meta-Analysis of Randomized Clinical Trials
Abstract
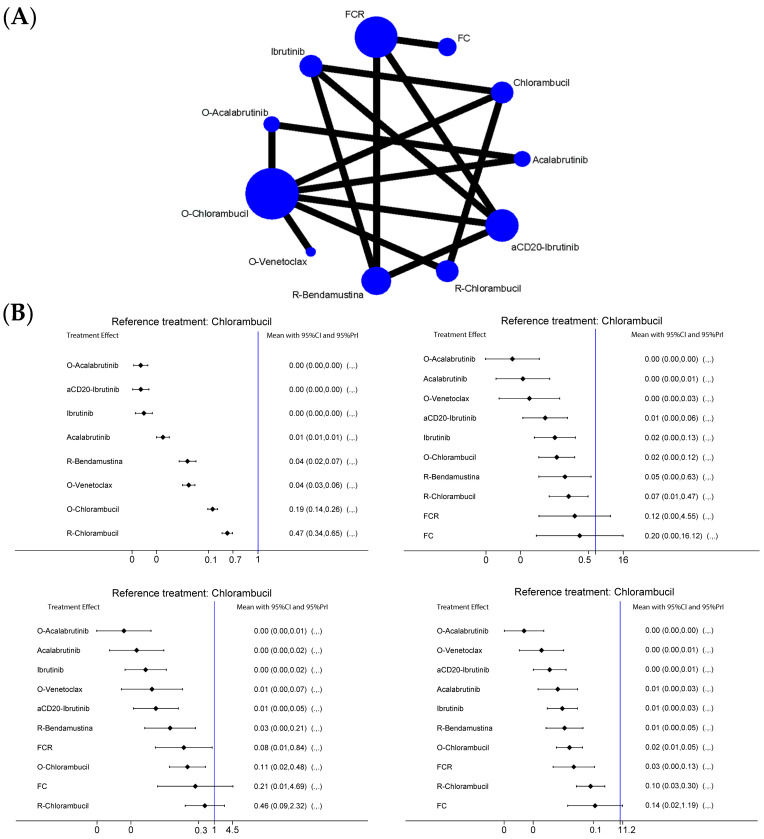
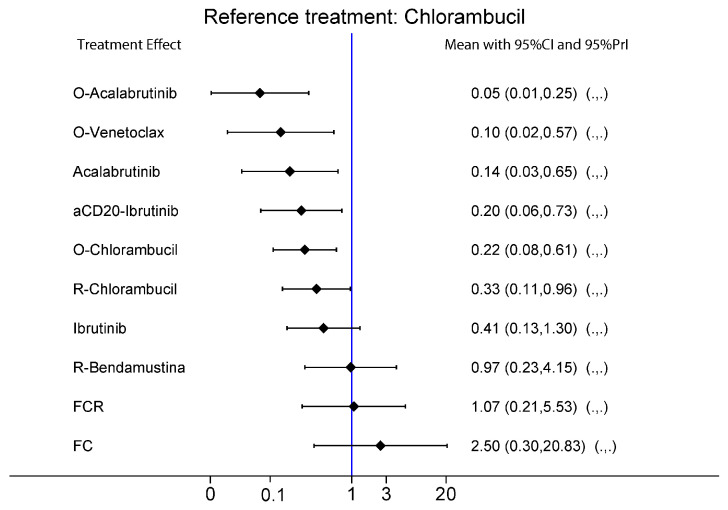
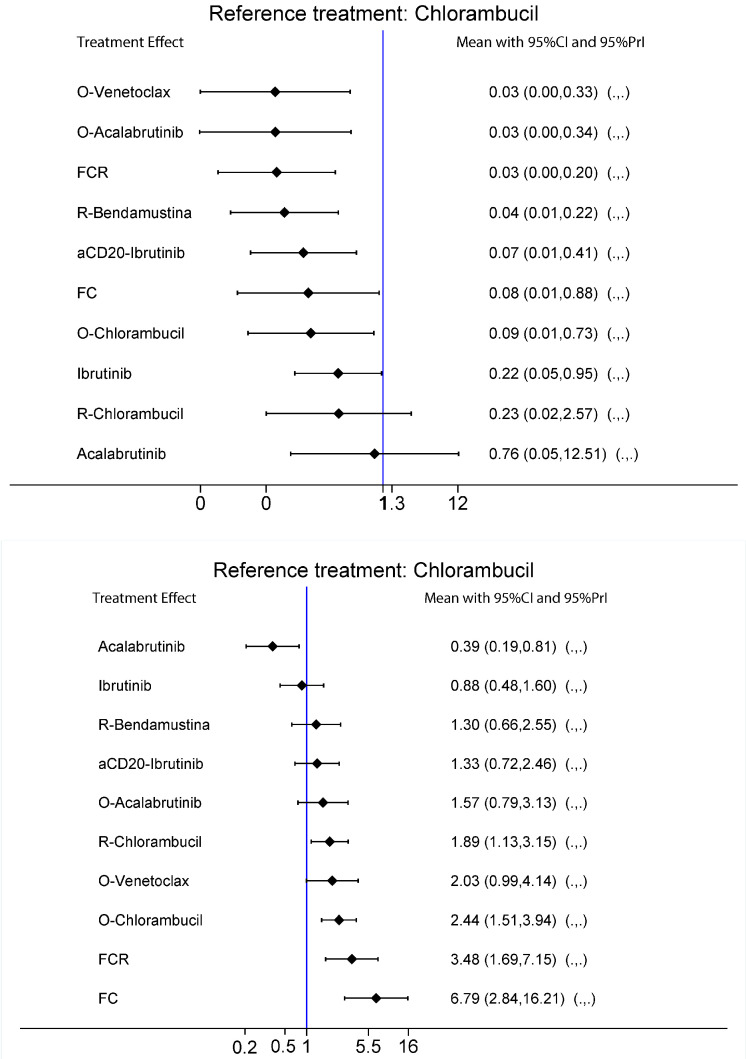
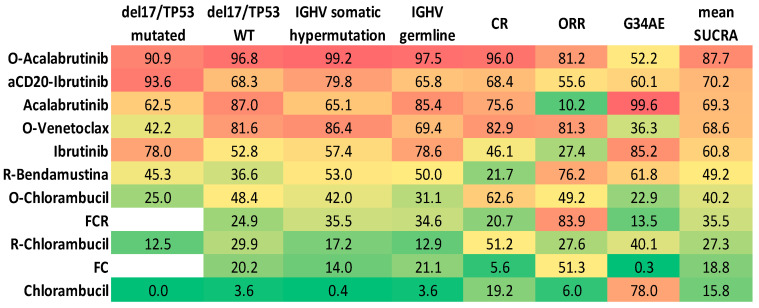
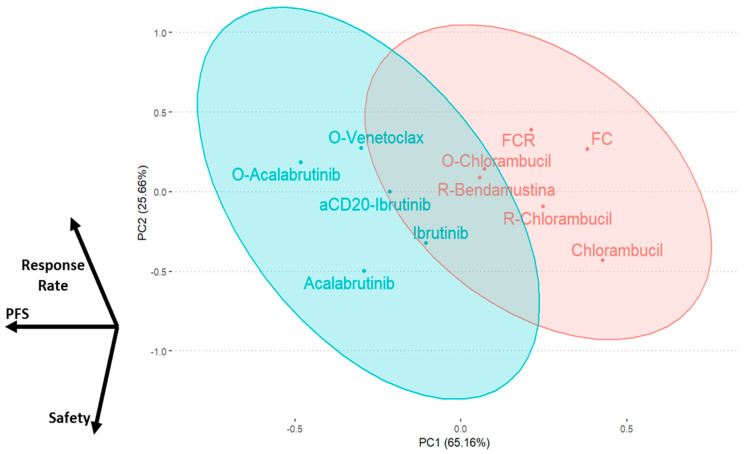
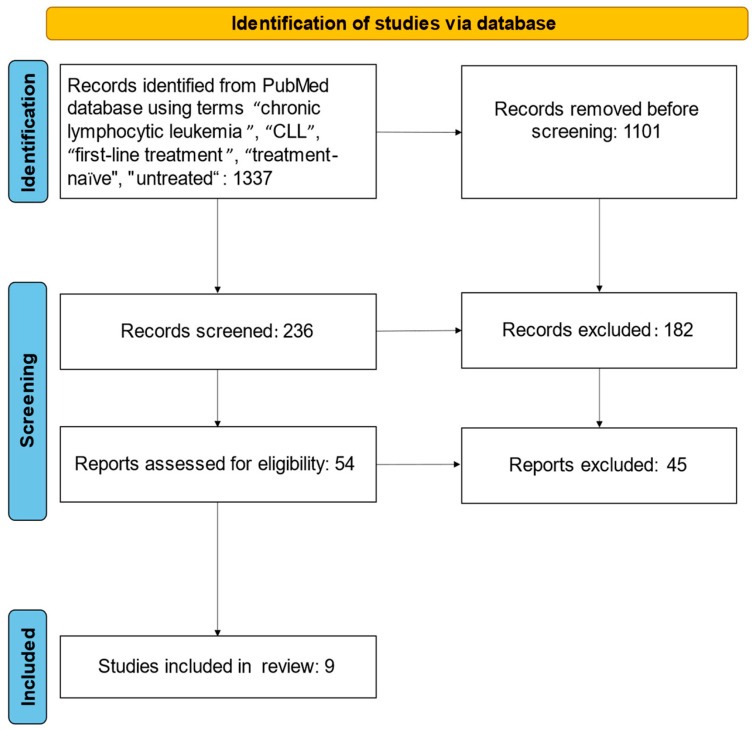
The treatment of chronic lymphocytic leukemia (CLL) currently relies on the use of chemo-immunotherapy, Bruton's tyrosine kinase inhibitors, or BCL2 inhibitors alone or combined with an anti-CD20 monoclonal antibody. However, the availability of multiple choices for the first-line setting and a lack of direct head-to-head comparisons pose a challenge for treatment selection. To overcome these limitations, we performed a systematic review and a network meta-analysis on published randomized clinical trials performed in the first-line treatment setting of CLL. For each study, we retrieved data on progression-free survival (according to del17/P53 and IGHV status), overall response rate, complete response, and incidence of most frequent grade 3-4 adverse event. We identified nine clinical trials encompassing 11 different treatments, with a total of 5288 CLL patients evaluated. We systematically performed separated network meta-analyses (NMA) to evaluate the efficacy/safety of each regimen in the conditions previously described to obtain the surface under the cumulative ranking curve (SUCRA) score, which was subsequently used to build separated ranking charts. Interestingly, the combination of obinutuzumab with acalabrutinib reached the top of the chart in each sub-analysis performed, with the exception of the del17/P53mut setting, where it was almost on par with the aCD20 mAbs/ibrutinib combination (SUCRA aCD20-ibrutinib and O-acala: 93.5% and 91%, respectively) and of the safety evaluation, where monotherapies (acalabrutinib in particular) gave better results. Finally, considering that NMA and SUCRA work for single endpoints only, we performed a principal component analysis to recapitulate in a cartesian plane the SUCRA profiles of each schedule according to the results obtained in each sub-analysis, confirming again the superiority of aCD20/BTKi or BCL2i combinations in a first-line setting. Overall, here we demonstrated that: (1) a chemotherapy-free regimen, such as the combination of aCD20 with a BTKi or BCL2i, should be the preferred treatment choice despite biological/molecular characteristics (preferred regimen O-acala); (2) there is less and less room for chemotherapy in the first line treatment of CLL.
Keywords: Bruton’s tyrosine kinase inhibitors; CLL; chronic lymphocitic leukemia; network metanalysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Dighiero G., Binet J.L. Chronic lymphocytic leukemia. Hematol. Cell Ther. 1996;38((Suppl. S2)):S41–S61. - PubMed
-
- Chronic Lymphocytic Leukemia—Cancer Stat Facts. [(accessed on 7 July 2022)]; Available online: https://seer.cancer.gov/statfacts/html/clyl.html.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
