

Pulmonary Hypertension in Left Heart Diseases: Pathophysiology, Hemodynamic Assessment and Therapeutic Management
- PMID: 37373119
- PMCID: PMC10298585
- DOI: 10.3390/ijms24129971
Pulmonary Hypertension in Left Heart Diseases: Pathophysiology, Hemodynamic Assessment and Therapeutic Management
Abstract
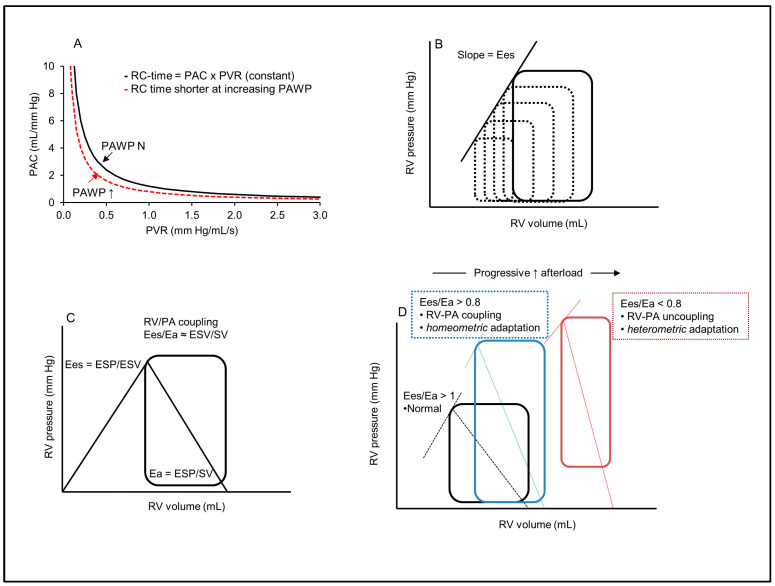
Pulmonary hypertension (PH) associated with left heart diseases (PH-LHD), also termed group 2 PH, represents the most common form of PH. It develops through the passive backward transmission of elevated left heart pressures in the setting of heart failure, either with preserved (HFpEF) or reduced (HFrEF) ejection fraction, which increases the pulsatile afterload of the right ventricle (RV) by reducing pulmonary artery (PA) compliance. In a subset of patients, progressive remodeling of the pulmonary circulation resulted in a pre-capillary phenotype of PH, with elevated pulmonary vascular resistance (PVR) further increasing the RV afterload, eventually leading to RV-PA uncoupling and RV failure. The primary therapeutic objective in PH-LHD is to reduce left-sided pressures through the appropriate use of diuretics and guideline-directed medical therapies for heart failure. When pulmonary vascular remodeling is established, targeted therapies aiming to reduce PVR are theoretically appealing. So far, such targeted therapies have mostly failed to show significant positive effects in patients with PH-LHD, in contrast to their proven efficacy in other forms of pre-capillary PH. Whether such therapies may benefit some specific subgroups of patients (HFrEF, HFpEF) with specific hemodynamic phenotypes (post- or pre-capillary PH) and various degrees of RV dysfunction still needs to be addressed.
Keywords: left heart disease; pathophysiology; pulmonary hypertension; therapeutics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Left ventricular heart failure and pulmonary hypertension.Eur Heart J. 2016 Mar 21;37(12):942-54. doi: 10.1093/eurheartj/ehv512. Epub 2015 Oct 27. Eur Heart J. 2016. PMID: 26508169 Free PMC article. Review.
-
Pulmonary hypertension in HFpEF and HFrEF: Pathophysiology, diagnosis, treatment approaches.Herz. 2019 Sep;44(6):483-490. doi: 10.1007/s00059-019-4831-6. Herz. 2019. PMID: 31317203 English.
-
A Model of Reverse Vascular Remodeling in Pulmonary Hypertension Due to Left Heart Disease by Aortic Debanding in Rats.J Vis Exp. 2022 Mar 1;(181). doi: 10.3791/63502. J Vis Exp. 2022. PMID: 35311828
-
Updates in the Pharmacotherapy of Pulmonary Hypertension in Patients with Heart Failure with Preserved Ejection Fraction.Cardiovasc Hematol Disord Drug Targets. 2023;23(4):215-225. doi: 10.2174/011871529X258234230921112507. Cardiovasc Hematol Disord Drug Targets. 2023. PMID: 37921162
-
Pulmonary hypertension due to left heart diseases.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D100-8. doi: 10.1016/j.jacc.2013.10.033. J Am Coll Cardiol. 2013. PMID: 24355634 Review.
Cited by
-
Editorial: Model organisms in experimental pharmacology and drug discovery 2023: rodent, worm and zebrafish models.Front Pharmacol. 2024 Aug 8;15:1462972. doi: 10.3389/fphar.2024.1462972. eCollection 2024. Front Pharmacol. 2024. PMID: 39175535 Free PMC article. No abstract available.
-
Hemodynamic Definitions, Phenotypes, Pathophysiology, and Evaluation of Pulmonary Hypertension Related to Left Heart Disease.J Cardiovasc Dev Dis. 2025 Jun 22;12(7):238. doi: 10.3390/jcdd12070238. J Cardiovasc Dev Dis. 2025. PMID: 40710764 Free PMC article. Review.
-
The Hidden Price of Plenty: Oxidative Stress and Calorie-Induced Cardiometabolic Dysfunction.Life (Basel). 2025 Jun 27;15(7):1022. doi: 10.3390/life15071022. Life (Basel). 2025. PMID: 40724524 Free PMC article. Review.
-
Is Inducible Nitric Oxide Synthase (iNOS) Promising as a New Target Against Pulmonary Hypertension?Antioxidants (Basel). 2025 Mar 21;14(4):377. doi: 10.3390/antiox14040377. Antioxidants (Basel). 2025. PMID: 40298665 Free PMC article. Review.
-
Pressure Overload and Right Ventricular Failure: From Pathophysiology to Treatment.J Clin Med. 2023 Jul 17;12(14):4722. doi: 10.3390/jcm12144722. J Clin Med. 2023. PMID: 37510837 Free PMC article. Review.
References
-
- Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M.F., Brida M., Carlsen J., Coats A.J.S., Escribano-Subias P., Ferrari P., et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022;43:3618–3731. doi: 10.1093/eurheartj/ehac237. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
