

The Optimal Fluid Strategy Matters in Liver Surgery: A Retrospective Single Centre Analysis of 666 Consecutive Liver Resections
- PMID: 37373656
- PMCID: PMC10299667
- DOI: 10.3390/jcm12123962
The Optimal Fluid Strategy Matters in Liver Surgery: A Retrospective Single Centre Analysis of 666 Consecutive Liver Resections
Abstract
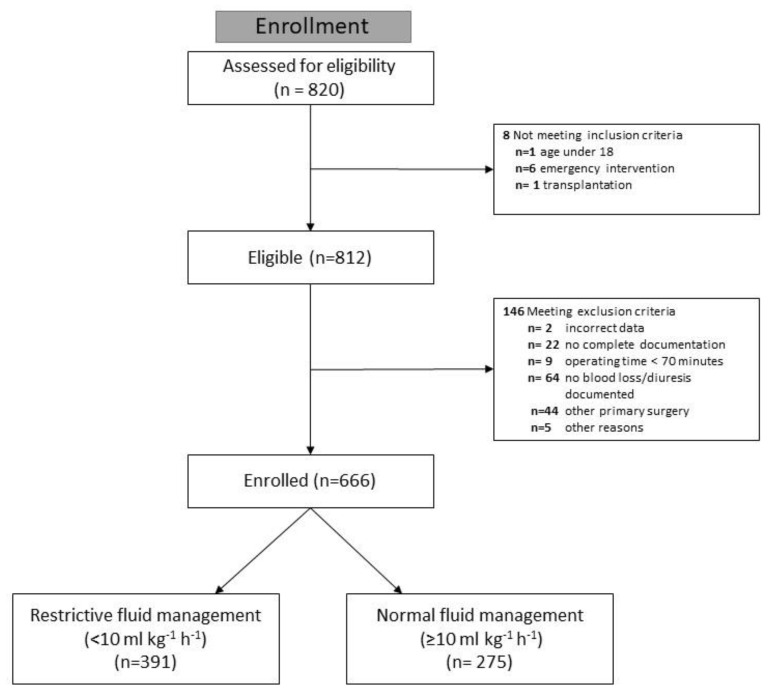
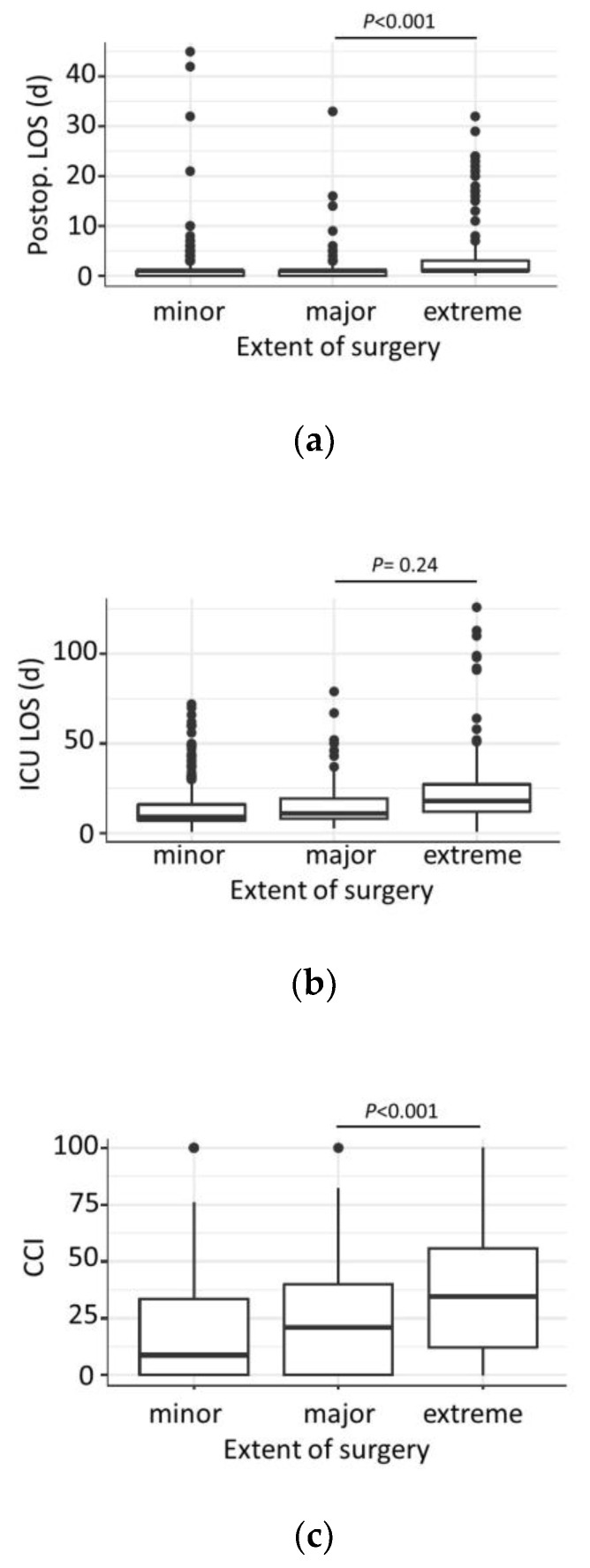
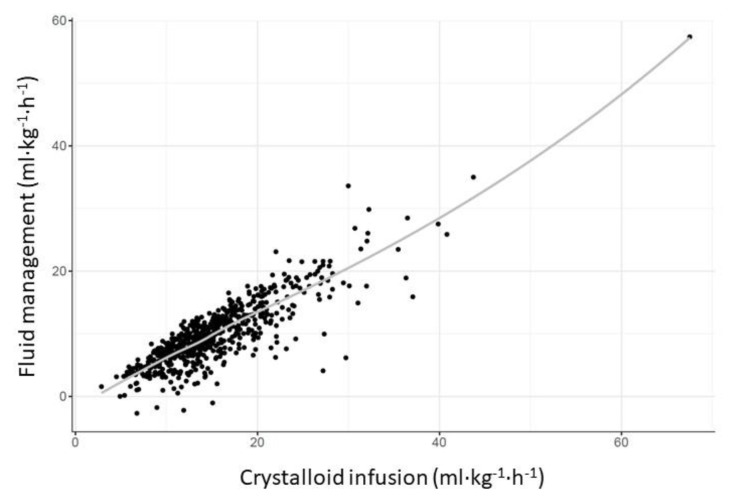
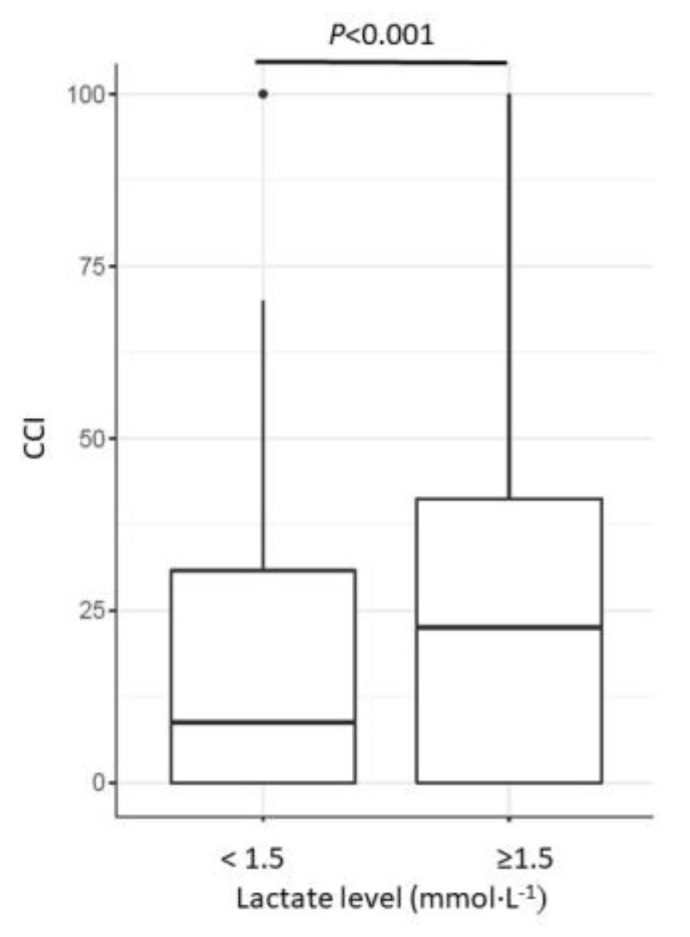
As optimal intraoperative fluid management in liver surgery has not been established, we retrospectively analyzed our fluid strategy in a high-volume liver surgery center in 666 liver resections. Intraoperative fluid management was divided into very restrictive (<10 m kg-1 h-1) and normal (≥10 mL kg-1 h-1) groups for study group characterization. The primary endpoint was morbidity as assessed by the Clavien-Dindo (CD) score and the comprehensive complication index (CCI). Logistic regression models identified factors most predictive of postoperative morbidity. No association was found between postoperative morbidity and fluid management in the overall study population (p = 0.89). However, the normal fluid management group had shorter postoperative hospital stays (p = <0.001), shorter ICU stays (p = 0.035), and lower in-hospital mortality (p = 0.02). Elevated lactate levels (p < 0.001), duration (p < 0.001), and extent of surgery (p < 0.001) were the most predictive factors for postoperative morbidity. In the subgroup of major/extreme liver resection, very low total (p = 0.028) and normalized fluid balance (p = 0.025) (NFB) were associated with morbidity. Moreover, fluid management was not associated with morbidity in patients with normal lactate levels (<2.5 mmol/L). In conclusion, fluid management in liver surgery is multifaceted and must be applied judiciously as a therapeutic measure. While a restrictive strategy appears attractive, hypovolemia should be avoided.
Keywords: adverse effects; fluid management; hepatectomy; intravenous infusion; surgical procedures.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Melloul E., Hübner M., Scott M., Snowden C., Prentis J., Dejong C.H., Garden O.J., Farges O., Kokudo N., Vauthey J.N., et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016;40:2425–2440. doi: 10.1007/s00268-016-3700-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
