

Mechanisms of Atrial Fibrillation: How Our Knowledge Affects Clinical Practice
- PMID: 37374043
- PMCID: PMC10303005
- DOI: 10.3390/life13061260
Mechanisms of Atrial Fibrillation: How Our Knowledge Affects Clinical Practice
Abstract
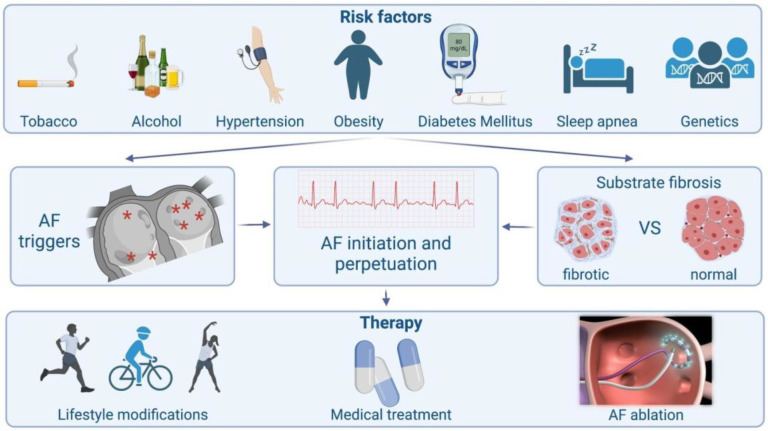
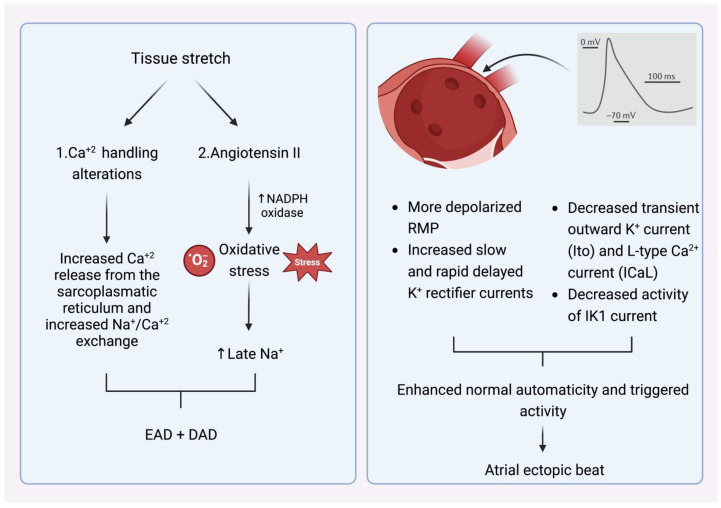
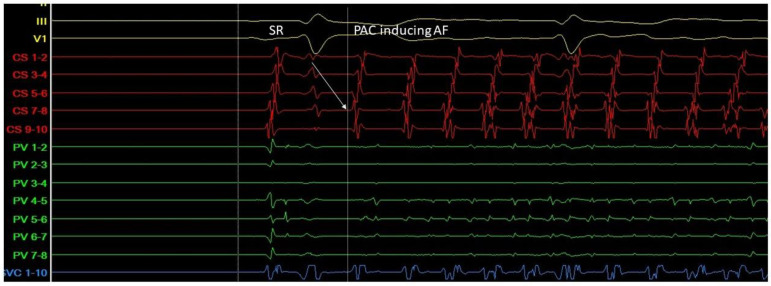
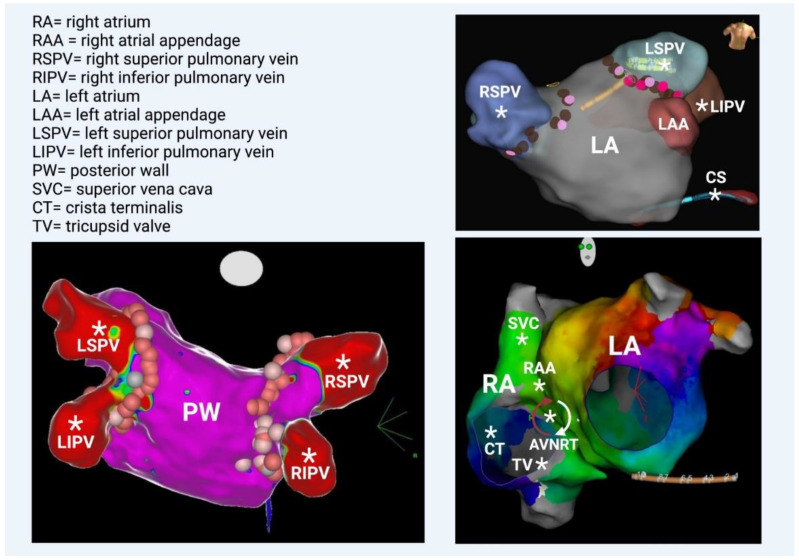
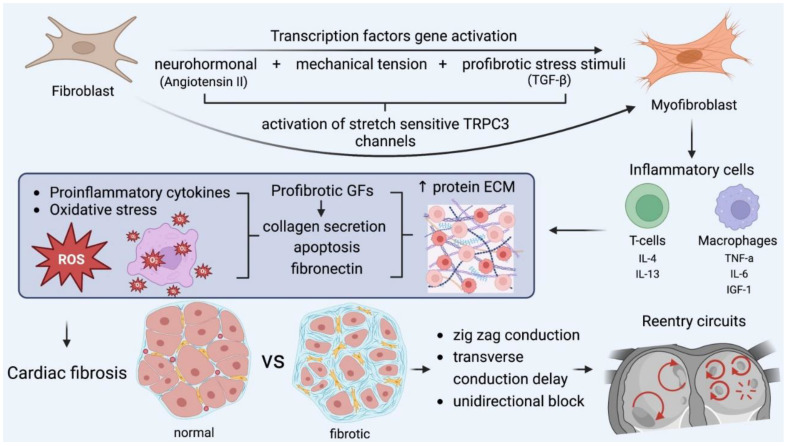
Atrial fibrillation (AF) is a very common arrhythmia that mainly affects older individuals. The mechanism of atrial fibrillation is complex and is related to the pathogenesis of trigger activation and the perpetuation of arrhythmia. The pulmonary veins in the left atrium arei confirm that onfirm the most common triggers due to their distinct anatomical and electrophysiological properties. As a result, their electrical isolation by ablation is the cornerstone of invasive AF treatment. Multiple factors and comorbidities affect the atrial tissue and lead to myocardial stretch. Several neurohormonal and structural changes occur, leading to inflammation and oxidative stress and, consequently, a fibrotic substrate created by myofibroblasts, which encourages AF perpetuation. Several mechanisms are implemented into daily clinical practice in both interventions in and the medical treatment of atrial fibrillation.
Keywords: atrial fibrillation; fibrosis; inflammation oxidative stress; triggers.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tsigkas G., Apostolos A., Despotopoulos S., Vasilagkos G., Kallergis E., Leventopoulos G., Mplani V., Davlouros P. Heart failure and atrial fibrillation: New concepts in pathophysiology, management, and future directions. Heart Fail. Rev. 2022;27:1201–1210. doi: 10.1007/s10741-021-10133-6. - DOI - PubMed
-
- Olshansky B., Goldberger Z.D., FACC. FHRS. Pogwizd S.M. The electrocardiogram in atrial. In: Knight B.P., Yeon S.B., editors. UpToDate. UpToDate; Waltham, MA, USA: 2021.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
