

Circumferential Pulmonary Vein Isolation With vs Without Additional Low-Voltage-Area Ablation in Older Patients With Paroxysmal Atrial Fibrillation: A Randomized Clinical Trial
- PMID: 37378966
- PMCID: PMC10308299
- DOI: 10.1001/jamacardio.2023.1749
Circumferential Pulmonary Vein Isolation With vs Without Additional Low-Voltage-Area Ablation in Older Patients With Paroxysmal Atrial Fibrillation: A Randomized Clinical Trial
Abstract
Importance: The overall success rate of circumferential pulmonary vein isolation (CPVI) treatment in patients with paroxysmal atrial fibrillation (AF) remains suboptimal, especially in older patients.
Objective: To explore the incremental benefit of low-voltage-area ablation after CPVI in older patients with paroxysmal AF.
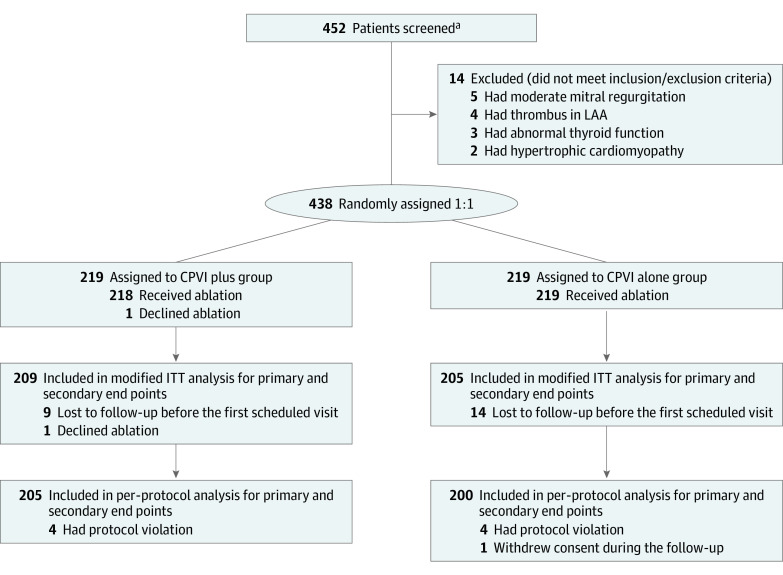
Design, setting, and participants: This randomized clinical trial was an investigator-initiated trial to compare the efficacy of additional low-voltage-area ablation beyond CPVI vs CPVI alone in older patients with paroxysmal AF. Participants were patients aged 65 to 80 years with paroxysmal AF who were referred for catheter ablation. They were enrolled in 14 tertiary hospitals in China from April 1, 2018, to August 3, 2020, and follow-up occurred through August 15, 2021.
Interventions: Patients were randomized (1:1) to undergo CPVI plus low-voltage-area ablation or CPVI alone. Low-voltage areas were defined as areas with amplitude less than 0.5 mV in more than 3 adjacent points. If low-voltage areas existed, additional substrate ablation was performed in the CPVI plus group but not the CPVI alone group.
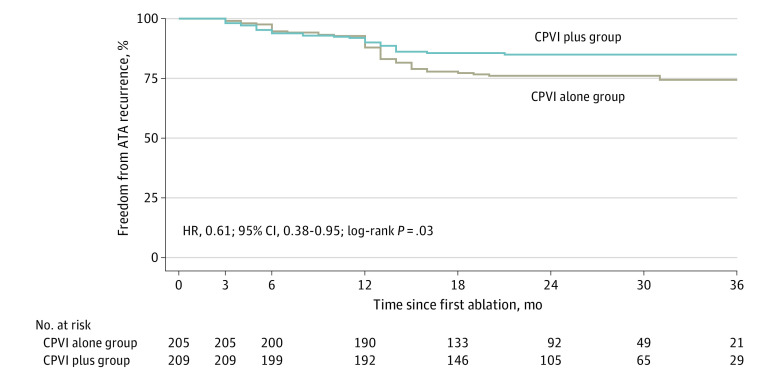
Main outcomes and measures: The primary end point of the study was freedom from atrial tachyarrhythmia as documented by electrocardiogram during a clinical visit or lasting longer than 30 seconds during Holter recordings occurring after a single ablation procedure.
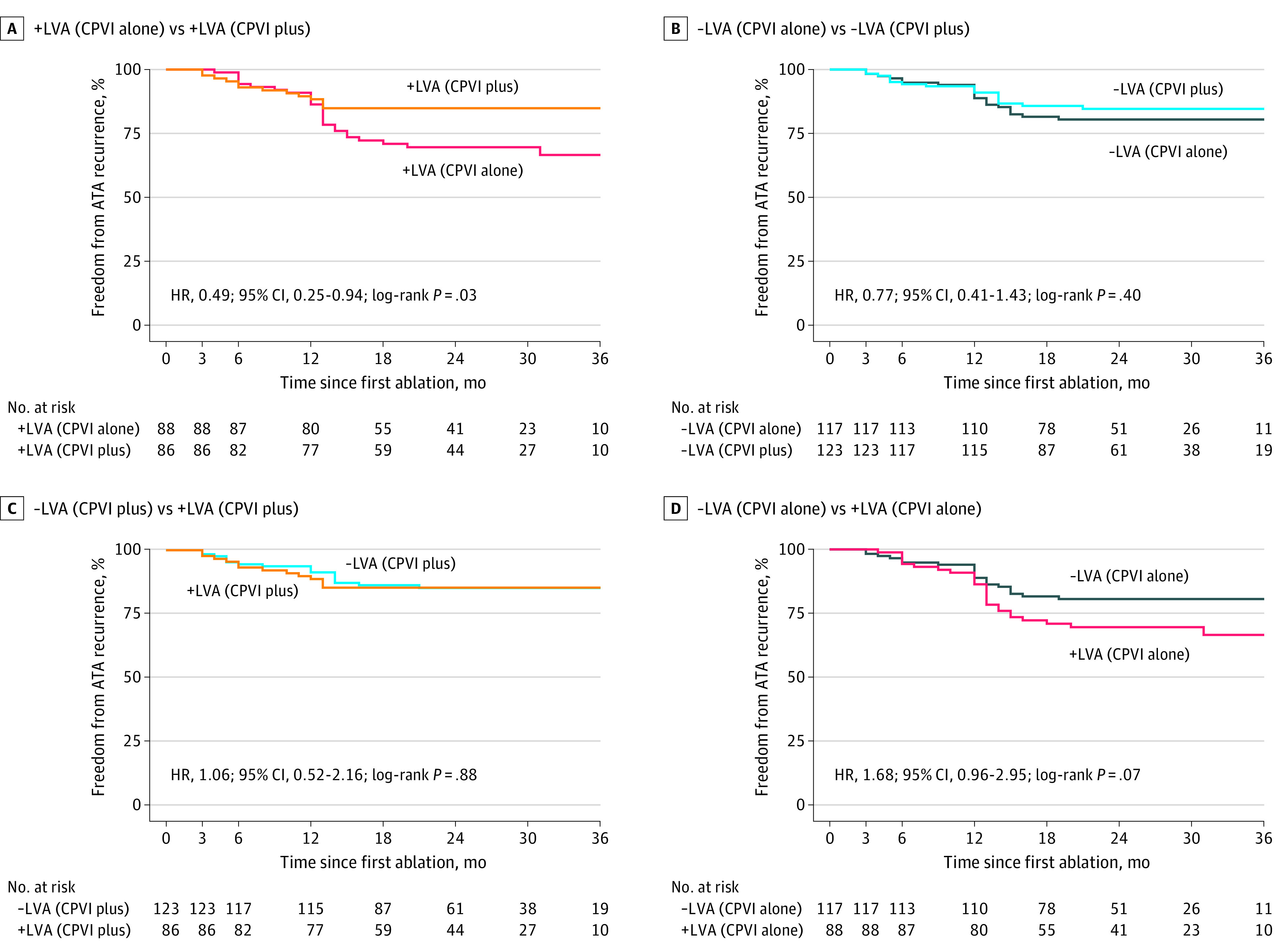
Results: Among 438 patients who were randomized (mean [SD] age, 70.5 [4.4] years; 219 men [50%]), 24 (5.5%) did not complete the blanking period and were not included for efficacy analysis. After a median follow-up of 23 months, the recurrence rate of atrial tachyarrhythmia was significantly lower in the CPVI plus group (31/209 patients, 15%) compared with the CPVI alone group (49/205, 24%; hazard ratio [HR], 0.61; 95% CI, 0.38-0.95; P = .03). In subgroup analyses, among all patients with low-voltage area, CPVI plus substrate modification was associated with a 51% decreased risk of ATA recurrence compared with CPVI alone (HR, 0.49; 95% CI, 0.25-0.94; P = .03).
Conclusions and relevance: This study found that additional low-voltage-area ablation beyond CPVI decreased the ATA recurrence in older patients with paroxysmal AF compared with CPVI alone. Our findings merit further replication by larger trials with longer follow-up.
Trial registration: ClinicalTrials.gov Identifier: NCT03462628.
Conflict of interest statement
Figures
Comment in
-
Gauging the Success of Low-Voltage-Area Ablation.JAMA Cardiol. 2023 Aug 1;8(8):773-774. doi: 10.1001/jamacardio.2023.1765. JAMA Cardiol. 2023. PMID: 37379008 No abstract available.
References
-
- Schreiber D, Rieger A, Moser F, Kottkamp H. Catheter ablation of atrial fibrillation with box isolation of fibrotic areas: lessons on fibrosis distribution and extent, clinical characteristics, and their impact on long-term outcome. J Cardiovasc Electrophysiol. 2017;28(9):971-983. doi:10.1111/jce.13278 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
