

Learning Curves of Minimally Invasive Distal Pancreatectomy in Experienced Pancreatic Centers
- PMID: 37378968
- PMCID: PMC10308297
- DOI: 10.1001/jamasurg.2023.2279
Learning Curves of Minimally Invasive Distal Pancreatectomy in Experienced Pancreatic Centers
Abstract
Importance: Understanding the learning curve of a new complex surgical technique helps to reduce potential patient harm. Current series on the learning curve of minimally invasive distal pancreatectomy (MIDP) are mostly small, single-center series, thus providing limited data.
Objective: To evaluate the length of pooled learning curves of MIDP in experienced centers.
Design, setting, and participants: This international, multicenter, retrospective cohort study included MIDP procedures performed from January 1, 2006, through June 30, 2019, in 26 European centers from 8 countries that each performed more than 15 distal pancreatectomies annually, with an overall experience exceeding 50 MIDP procedures. Consecutive patients who underwent elective laparoscopic or robotic distal pancreatectomy for all indications were included. Data were analyzed between September 1, 2021, and May 1, 2022.
Exposures: The learning curve for MIDP was estimated by pooling data from all centers.
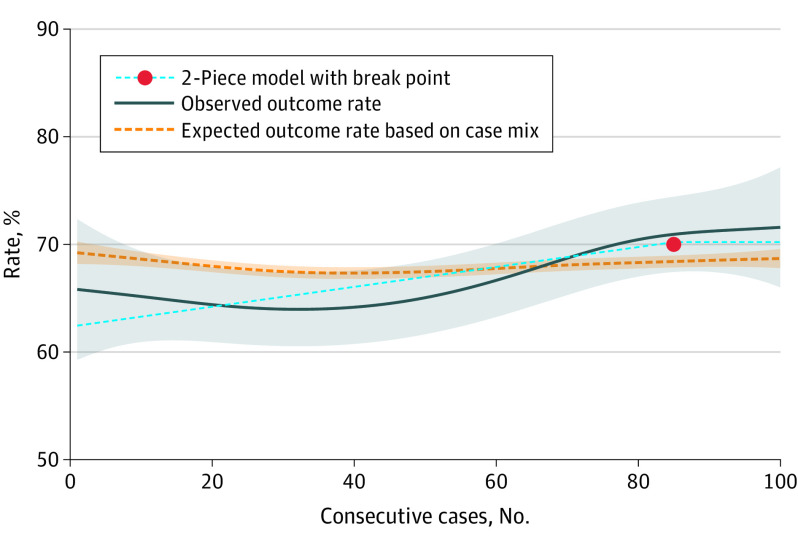
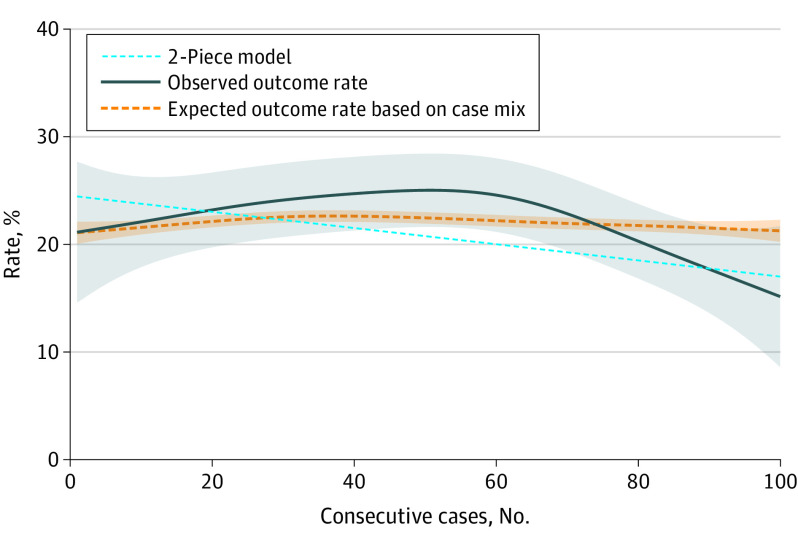
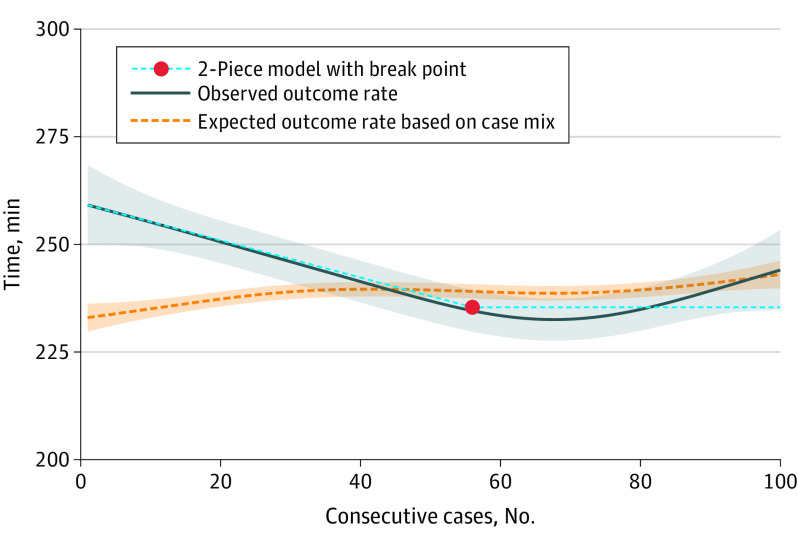
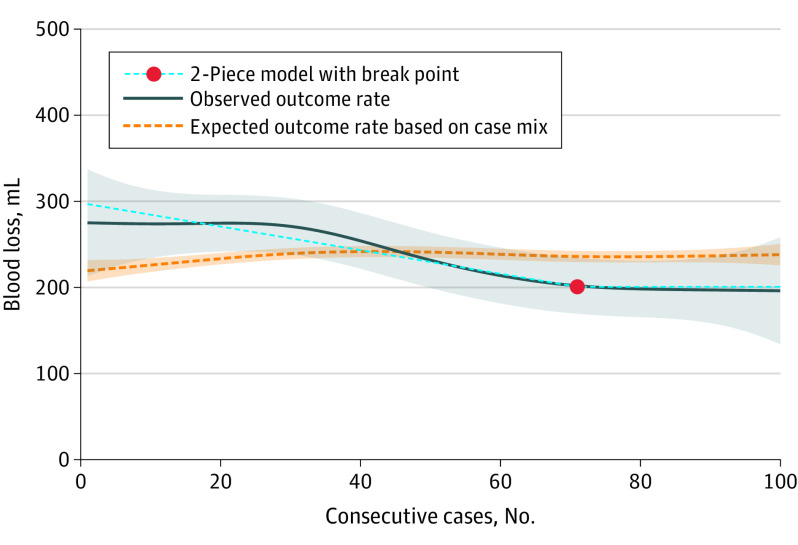
Main outcomes and measures: The learning curve was assessed for the primary textbook outcome (TBO), which is a composite measure that reflects optimal outcome, and for surgical mastery. Generalized additive models and a 2-piece linear model with a break point were used to estimate the learning curve length of MIDP. Case mix-expected probabilities were plotted and compared with observed outcomes to assess the association of changing case mix with outcomes. The learning curve also was assessed for the secondary outcomes of operation time, intraoperative blood loss, conversion to open rate, and postoperative pancreatic fistula grade B/C.
Results: From a total of 2610 MIDP procedures, the learning curve analysis was conducted on 2041 procedures (mean [SD] patient age, 58 [15.3] years; among 2040 with reported sex, 1249 were female [61.2%] and 791 male [38.8%]). The 2-piece model showed an increase and eventually a break point for TBO at 85 procedures (95% CI, 13-157 procedures), with a plateau TBO rate at 70%. The learning-associated loss of TBO rate was estimated at 3.3%. For conversion, a break point was estimated at 40 procedures (95% CI, 11-68 procedures); for operation time, at 56 procedures (95% CI, 35-77 procedures); and for intraoperative blood loss, at 71 procedures (95% CI, 28-114 procedures). For postoperative pancreatic fistula, no break point could be estimated.
Conclusion and relevance: In experienced international centers, the learning curve length of MIDP for TBO was considerable with 85 procedures. These findings suggest that although learning curves for conversion, operation time, and intraoperative blood loss are completed earlier, extensive experience may be needed to master the learning curve of MIDP.
Conflict of interest statement
Figures
Comment in
-
The Surgeon, the Center, and the System-Several Styles to Stage Mastery.JAMA Surg. 2023 Sep 1;158(9):934. doi: 10.1001/jamasurg.2023.2290. JAMA Surg. 2023. PMID: 37379051 No abstract available.
References
-
- de Rooij T, Jilesen AP, Boerma D, et al. A nationwide comparison of laparoscopic and open distal pancreatectomy for benign and malignant disease. J Am Coll Surg. 2015;220(3):263-270.e1. - PubMed
-
- Lof S, Moekotte AL, Al-Sarireh B, et al. ; Minimally Invasive Liver and Pancreatic Surgery Study Group - UK (MI-LAPS UK) . Multicentre observational cohort study of implementation and outcomes of laparoscopic distal pancreatectomy. Br J Surg. 2019;106(12):1657-1665. doi: 10.1002/bjs.11292 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
