

Coronary Atherosclerotic Plaque Activity and Future Coronary Events
- PMID: 37379010
- PMCID: PMC10308296
- DOI: 10.1001/jamacardio.2023.1729
Coronary Atherosclerotic Plaque Activity and Future Coronary Events
Abstract
Importance: Recurrent coronary events in patients with recent myocardial infarction remain a major clinical problem. Noninvasive measures of coronary atherosclerotic disease activity have the potential to identify individuals at greatest risk.
Objective: To assess whether coronary atherosclerotic plaque activity as assessed by noninvasive imaging is associated with recurrent coronary events in patients with myocardial infarction.
Design, setting, and participants: This prospective, longitudinal, international multicenter cohort study recruited participants aged 50 years or older with multivessel coronary artery disease and recent (within 21 days) myocardial infarction between September 2015 and February 2020, with a minimum 2 years' follow-up.
Intervention: Coronary 18F-sodium fluoride positron emission tomography and coronary computed tomography angiography.
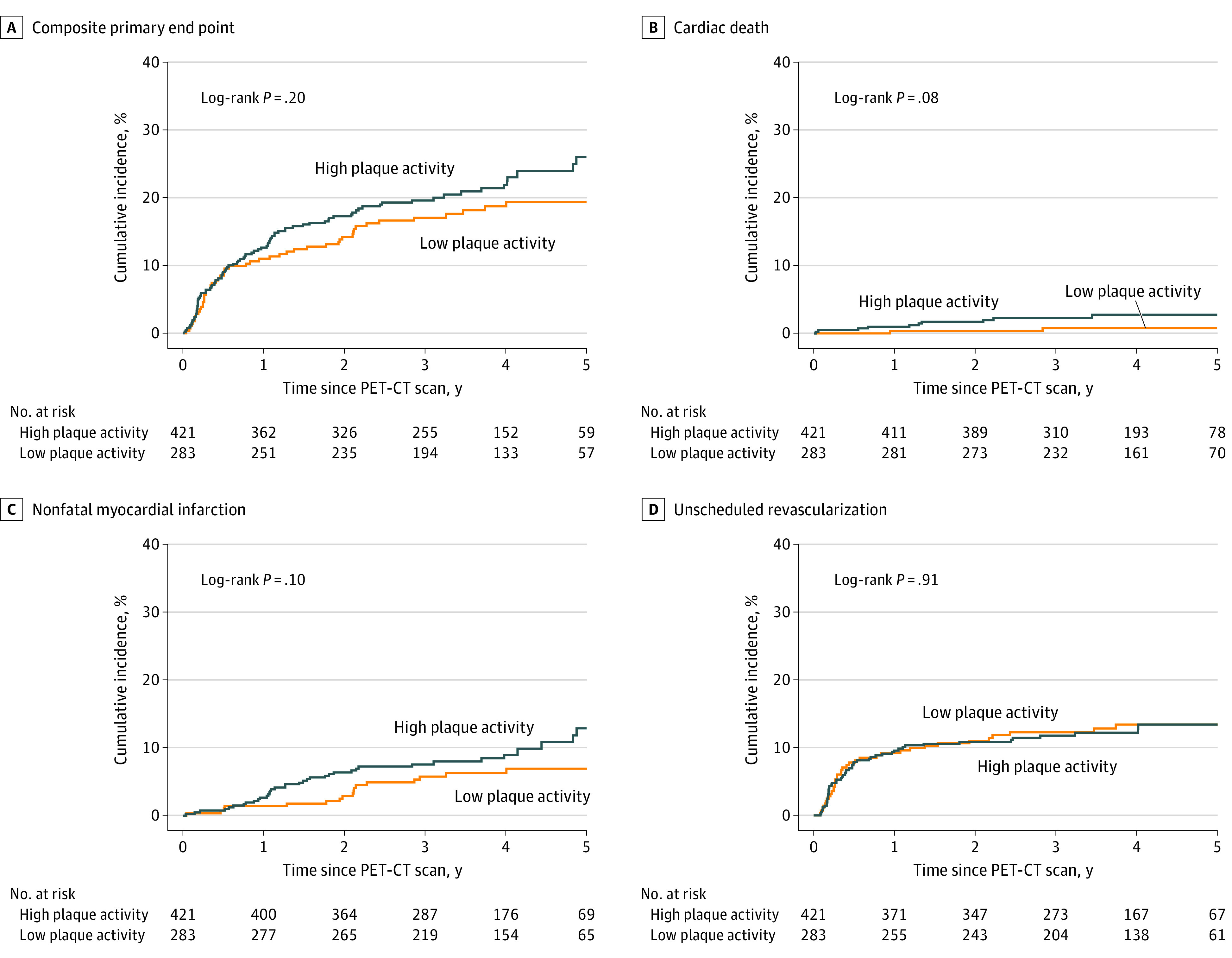
Main outcomes and measures: Total coronary atherosclerotic plaque activity was assessed by 18F-sodium fluoride uptake. The primary end point was cardiac death or nonfatal myocardial infarction but was expanded during study conduct to include unscheduled coronary revascularization due to lower than anticipated primary event rates.
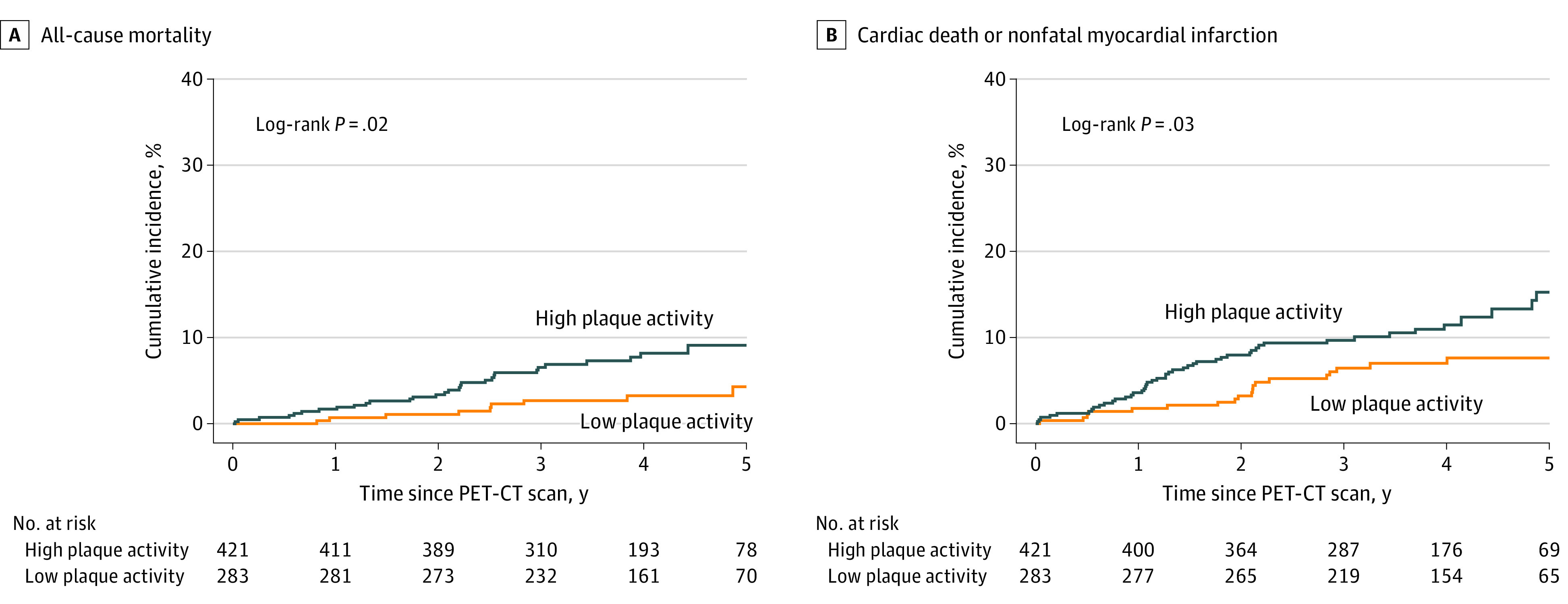
Results: Among 2684 patients screened, 995 were eligible, 712 attended for imaging, and 704 completed an interpretable scan and comprised the study population. The mean (SD) age of participants was 63.8 (8.2) years, and most were male (601 [85%]). Total coronary atherosclerotic plaque activity was identified in 421 participants (60%). After a median follow-up of 4 years (IQR, 3-5 years), 141 participants (20%) experienced the primary end point: 9 had cardiac death, 49 had nonfatal myocardial infarction, and 83 had unscheduled coronary revascularizations. Increased coronary plaque activity was not associated with the primary end point (hazard ratio [HR], 1.25; 95% CI, 0.89-1.76; P = .20) or unscheduled revascularization (HR, 0.98; 95% CI, 0.64-1.49; P = .91) but was associated with the secondary end point of cardiac death or nonfatal myocardial infarction (47 of 421 patients with high plaque activity [11.2%] vs 19 of 283 with low plaque activity [6.7%]; HR, 1.82; 95% CI, 1.07-3.10; P = .03) and all-cause mortality (30 of 421 patients with high plaque activity [7.1%] vs 9 of 283 with low plaque activity [3.2%]; HR, 2.43; 95% CI, 1.15-5.12; P = .02). After adjustment for differences in baseline clinical characteristics, coronary angiography findings, and Global Registry of Acute Coronary Events score, high coronary plaque activity was associated with cardiac death or nonfatal myocardial infarction (HR, 1.76; 95% CI, 1.00-3.10; P = .05) but not with all-cause mortality (HR, 2.01; 95% CI, 0.90-4.49; P = .09).
Conclusions and relevance: In this cohort study of patients with recent myocardial infarction, coronary atherosclerotic plaque activity was not associated with the primary composite end point. The findings suggest that risk of cardiovascular death or myocardial infarction in patients with elevated plaque activity warrants further research to explore its incremental prognostic implications.
Conflict of interest statement
Figures
Comment in
-
Can Noncalcified Plaques Contribute to Future Coronary Events?JAMA Cardiol. 2024 Jan 1;9(1):94. doi: 10.1001/jamacardio.2023.4390. JAMA Cardiol. 2024. PMID: 38019491 No abstract available.
References
-
- D’Ascenzo F, Biondi-Zoccai G, Moretti C, et al. TIMI, GRACE and alternative risk scores in acute coronary syndromes: a meta-analysis of 40 derivation studies on 216,552 patients and of 42 validation studies on 31,625 patients. Contemp Clin Trials. 2012;33(3):507-514. doi: 10.1016/j.cct.2012.01.001 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- PG/15/88/31780/BHF_/British Heart Foundation/United Kingdom
- MR/V007254/1/MRC_/Medical Research Council/United Kingdom
- CH/F/21/90010/BHF_/British Heart Foundation/United Kingdom
- DH_/Department of Health/United Kingdom
- FS/RTF/20/30009/BHF_/British Heart Foundation/United Kingdom
- RG/20/10/34966/BHF_/British Heart Foundation/United Kingdom
- AA/18/3/34220/BHF_/British Heart Foundation/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- R35 HL161195/HL/NHLBI NIH HHS/United States
- R01 HL135557/HL/NHLBI NIH HHS/United States
- PG/15/117/31961/BHF_/British Heart Foundation/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- PG/17/64/33205/BHF_/British Heart Foundation/United Kingdom
- NH/19/1/34595/BHF_/British Heart Foundation/United Kingdom
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- R01 HL148787/HL/NHLBI NIH HHS/United States
- PG/18/35/33786/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- FS/SCRF/21/32010/BHF_/British Heart Foundation/United Kingdom
- FS/ICRF/20/26002/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/BHF_/British Heart Foundation/United Kingdom
