

Subclonal TP53 mutations are frequent and predict resistance to radioimmunotherapy in follicular lymphoma
- PMID: 37379264
- PMCID: PMC10471938
- DOI: 10.1182/bloodadvances.2022009467
Subclonal TP53 mutations are frequent and predict resistance to radioimmunotherapy in follicular lymphoma
Abstract
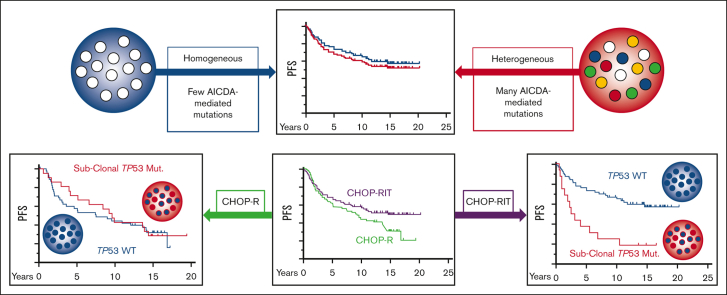
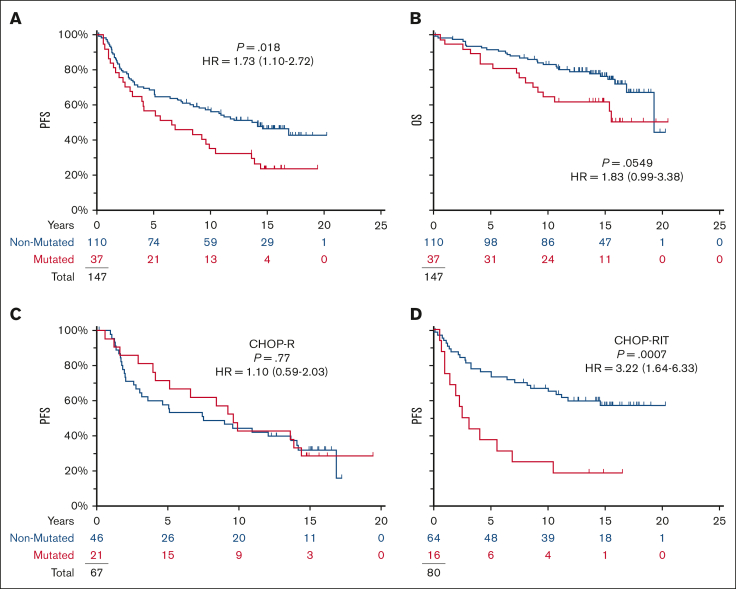
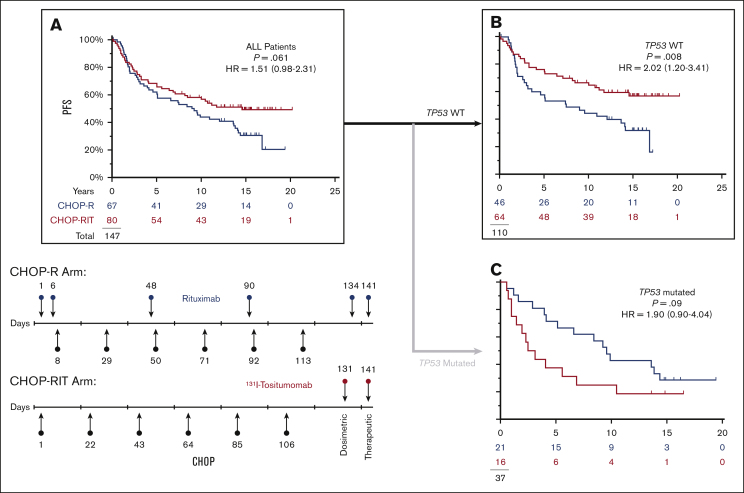
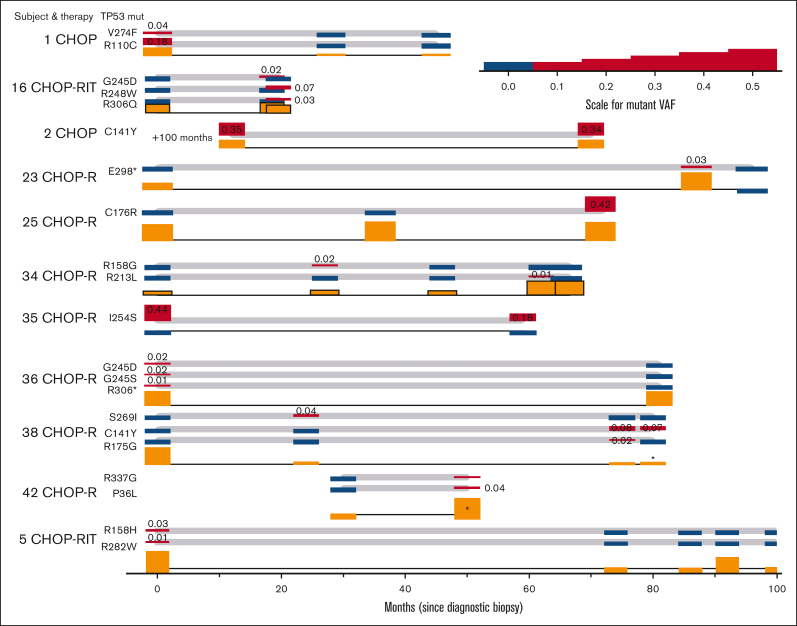
Although TP53 is commonly mutated in transformed follicular lymphoma, mutations are reported in <5% of pretreatment follicular lymphoma (FL) specimens. We assayed archival follicular B-cell non-Hodgkin lymphoma specimens from a completed clinical trial, Southwest Oncology Group S0016, a phase 3 randomized intergroup trial of CHOP (cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisone) chemotherapy plus R-CHOP (rituximab-CHOP) compared with CHOP chemotherapy plus 131-iodine tositumomab (radioimmunotherapy [RIT]-CHOP). Subclonal TP53 mutations (median allele frequency 0.02) were found in 25% of diagnostic FL specimens and in 27% of a separate validation cohort. In the R-CHOP arm, pathogenic TP53 mutations were not associated with progression-free survival (PFS) (10-year PFS 43% vs 44%). In contrast, among patients with no detectable pathogenic TP53 mutation, RIT-CHOP was associated with a longer PFS than with R-CHOP (10-year PFS 67% vs 44%; hazard ratio = 0.49; P = .008). No relationship was detected between PFS and the extent of activation-induced cytidine deaminase (AICDA)-mediated heterogeneity. In summary, subclonal TP53 mutations are common in FL and are a distinct phenomenon from AICDA-mediated genetic heterogeneity. The absence of a detectable subclonal mutation in TP53 defined a population that particularly benefited from RIT.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures

References
-
- Pasqualucci L. Molecular pathogenesis of germinal center-derived B cell lymphomas. Immunol Rev. 2019;288(1):240–261. - PubMed
-
- Pasqualucci L, Bhagat G, Jankovic M, et al. AID is required for germinal center-derived lymphomagenesis. Nat Genet. 2008;40(1):108–112. - PubMed
-
- Casulo C, Burack WR, Friedberg JW. Transformed follicular non-Hodgkin lymphoma. Blood. 2015;125(1):40–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
