

Using mortuary and burial data to place COVID-19 in Lusaka, Zambia within a global context
- PMID: 37380650
- PMCID: PMC10307769
- DOI: 10.1038/s41467-023-39288-6
Using mortuary and burial data to place COVID-19 in Lusaka, Zambia within a global context
Erratum in
-
Author Correction: Using mortuary and burial data to place COVID-19 in Lusaka, Zambia within a global context.Nat Commun. 2024 Mar 12;15(1):2213. doi: 10.1038/s41467-024-44940-w. Nat Commun. 2024. PMID: 38472189 Free PMC article. No abstract available.
Abstract
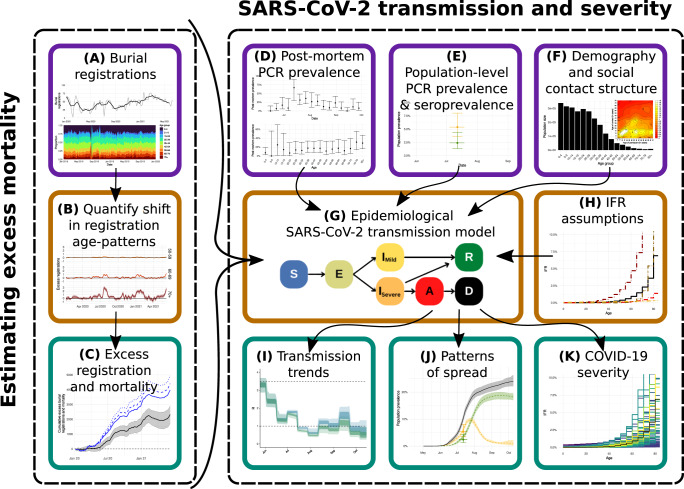
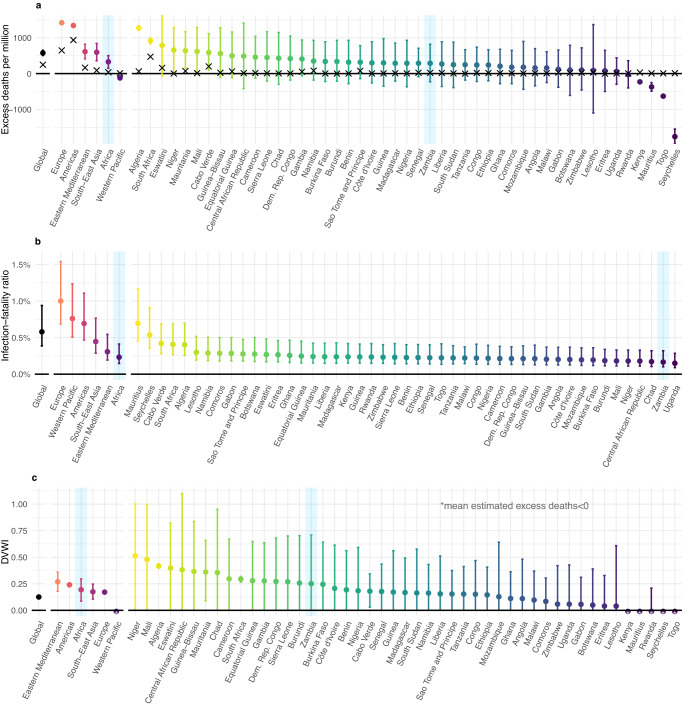
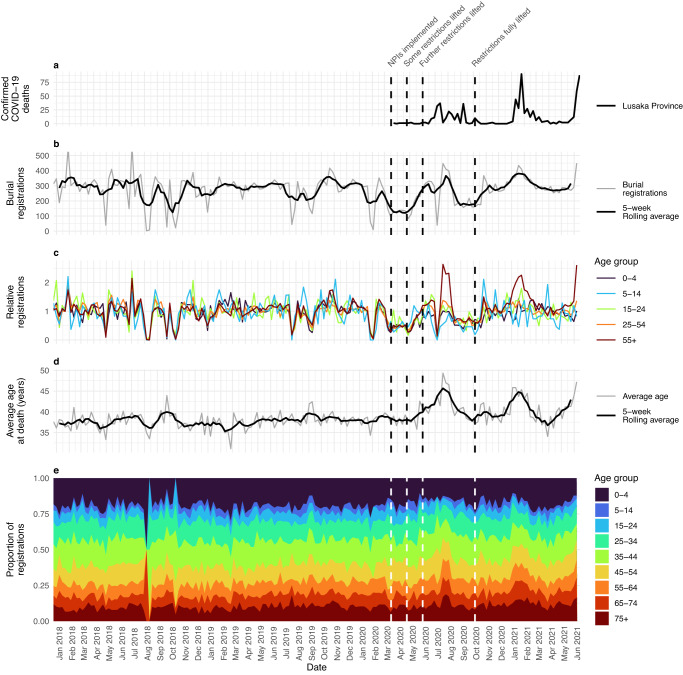
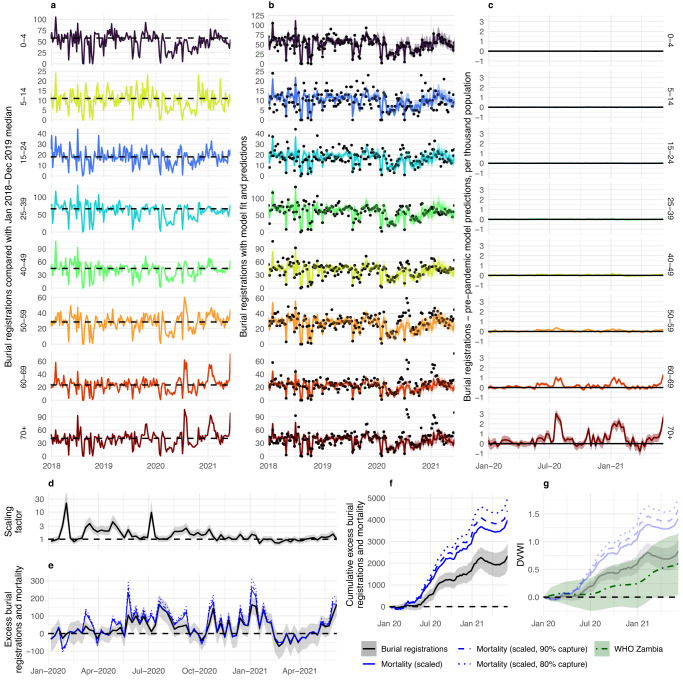
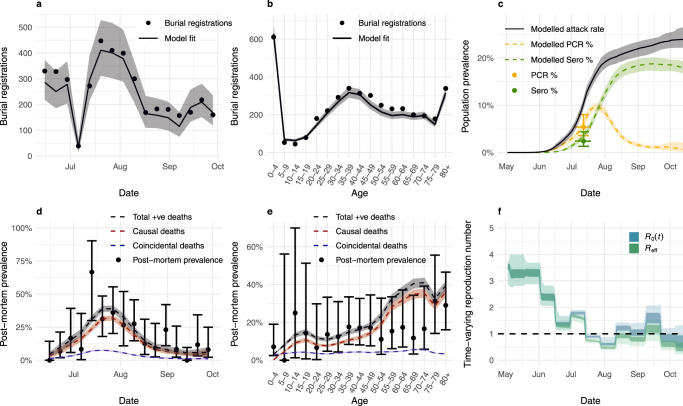
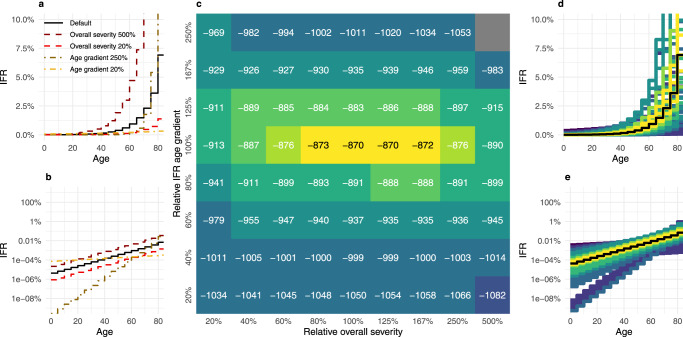
Reported COVID-19 cases and associated mortality remain low in many sub-Saharan countries relative to global averages, but true impact is difficult to estimate given limitations around surveillance and mortality registration. In Lusaka, Zambia, burial registration and SARS-CoV-2 prevalence data during 2020 allow estimation of excess mortality and transmission. Relative to pre-pandemic patterns, we estimate age-dependent mortality increases, totalling 3212 excess deaths (95% CrI: 2104-4591), representing an 18.5% (95% CrI: 13.0-25.2%) increase relative to pre-pandemic levels. Using a dynamical model-based inferential framework, we find that these mortality patterns and SARS-CoV-2 prevalence data are in agreement with established COVID-19 severity estimates. Our results support hypotheses that COVID-19 impact in Lusaka during 2020 was consistent with COVID-19 epidemics elsewhere, without requiring exceptional explanations for low reported figures. For more equitable decision-making during future pandemics, barriers to ascertaining attributable mortality in low-income settings must be addressed and factored into discourse around reported impact differences.
© 2023. The Author(s).
Conflict of interest statement
S.G. declares shareholdings in pharmaceutical companies (AstraZeneca and GlaxoSmithklineBeecham). L.C.O. declares grant funding for other projects from Merck Ltd. The remaining authors declare no competing interests.
Figures
References
-
- Global Economic Effects of COVID-19. https://apps.dtic.mil/sti/citations/AD1152929.
-
- WHO. WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. https://covid19.who.int/?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQiA4Oy... (2022).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
