

Watch brain circulation in unexplained progressive myelopathy: a review of Cognard type V arterio-venous fistulas
- PMID: 37380820
- PMCID: PMC10495521
- DOI: 10.1007/s10072-023-06870-1
Watch brain circulation in unexplained progressive myelopathy: a review of Cognard type V arterio-venous fistulas
Abstract
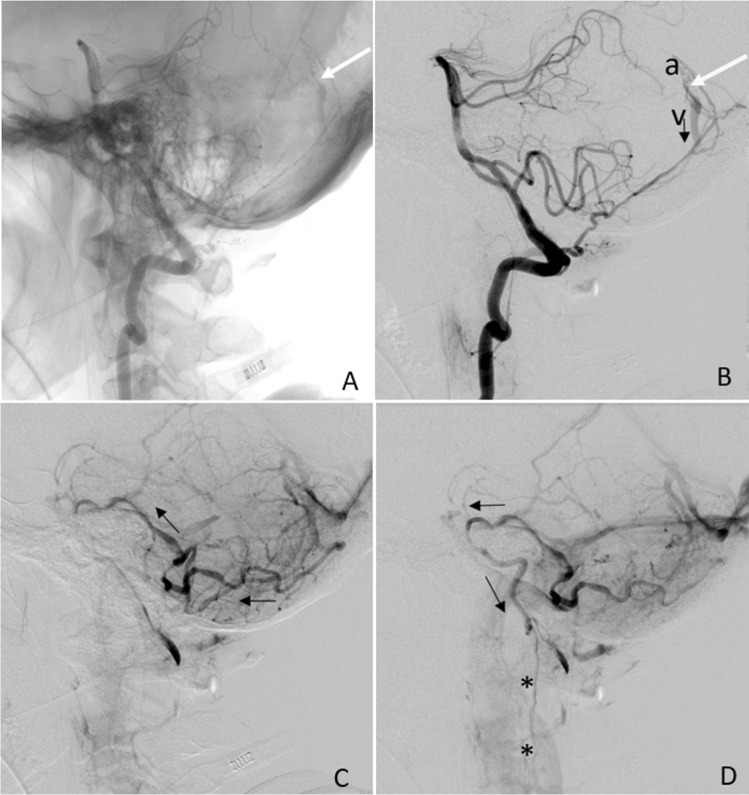
Background: Intracranial dural arterio-venous fistulas are pathological anastomoses between arteries and veins located within dural sheets and whose clinical manifestations depend on location and hemodynamic features. They can sometimes display perimedullary venous drainage (Cognard type V fistulas-CVFs) and present as a progressive myelopathy. Our review aims at describing CVFs' variety of clinical presentation, investigating a possible association between diagnostic delay and outcome and assessing whether there is a correlation between clinical and/or radiological signs and clinical outcomes.
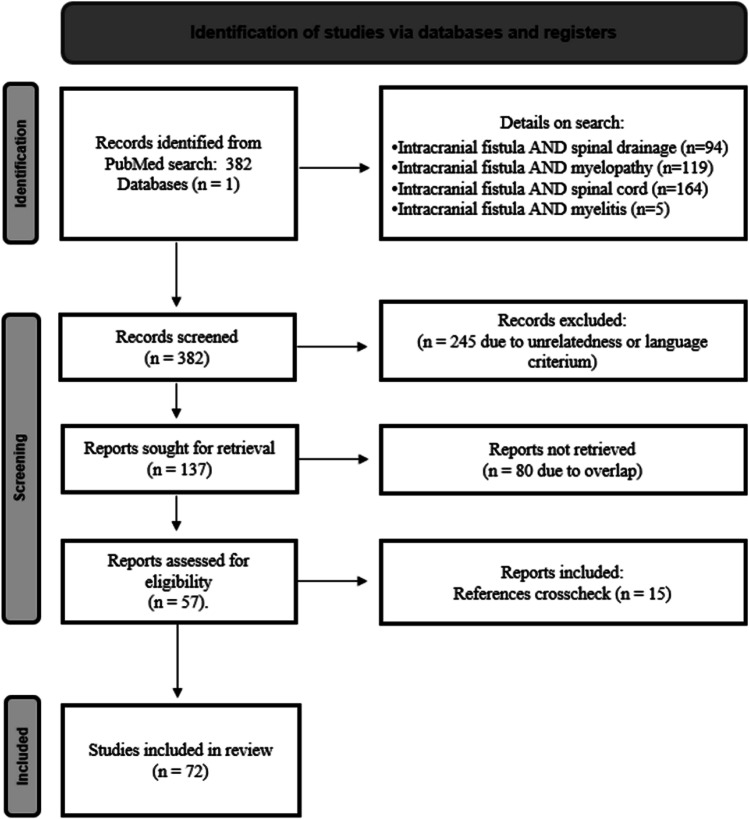
Methods: We conducted a systematic search on Pubmed, looking for articles describing patients with CVFs complicated with myelopathy.
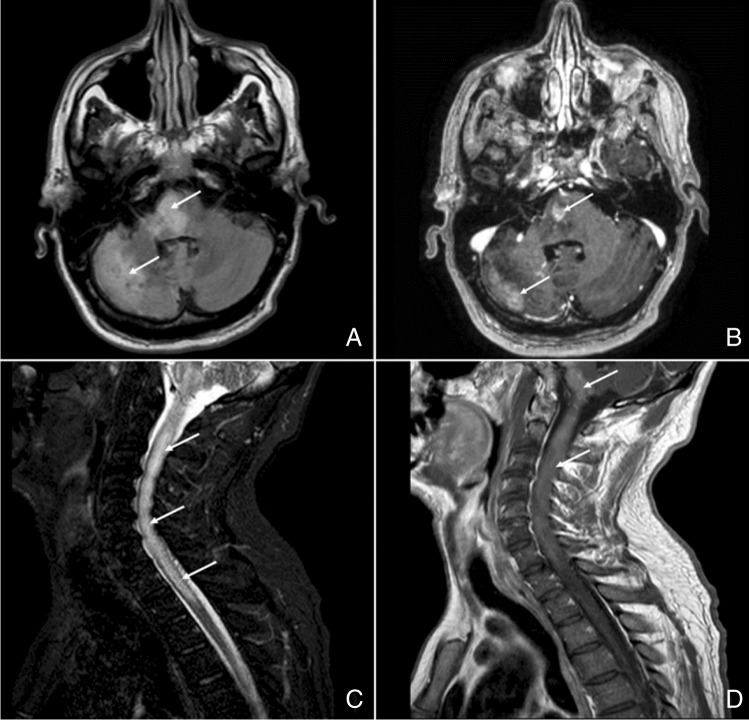
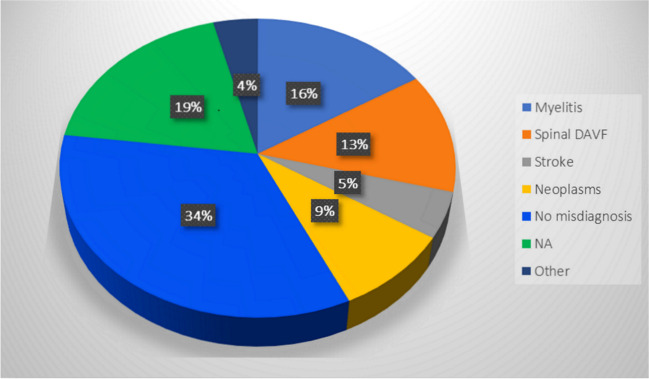
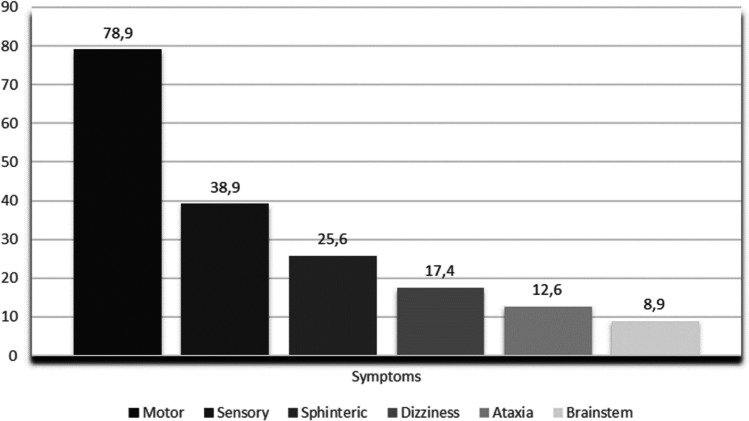
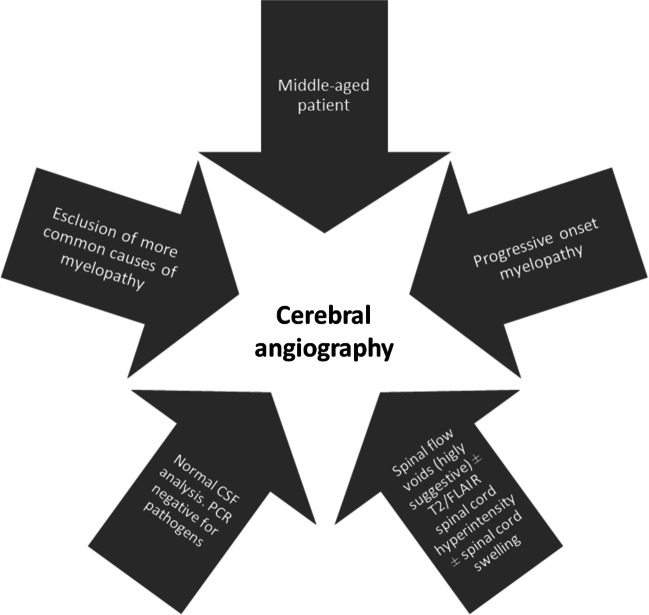
Results: A total of 72 articles for an overall of 100 patients were selected. The mean age was 56.20 ± 14.07, 72% of patients were man, and 58% received an initial misdiagnosis. CVFs showed a progressive onset in 65% of cases, beginning with motor symptoms in 79% of cases. As for the MRI, 81% presented spinal flow voids. The median time from symptoms' onset to diagnosis was 5 months with longer delays for patients experiencing worse outcomes. Finally, 67.1% of patients showed poor outcomes while the remaining 32.9% obtained a partial-to-full recovery.
Conclusions: We confirmed CVFs' broad clinical spectrum of presentation and found that the outcome is not associated with the severity of the clinical picture at onset, but it has a negative correlation with the length of diagnostic delay. We furthermore underlined the importance of cervico-dorsal perimedullary T1/T2 flow voids as a reliable MRI parameter to orient the diagnosis and distinguish CVFs from most of their mimics.
Keywords: Intracranial dural arterio-venous fistulas (iDAVFs); Intracranial vascular malformations; Myelopathy; Spinal cord disease.
© 2023. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Signorelli F. Intracranial dural arteriovenous fistulas: a review. J Neurol Stroke. 2014;1:35–40. doi: 10.15406/jnsk.2014.01.00007. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
