

Boost modalities in cervical cancer: dosimetric comparison between intracavitary BT vs. intracavitary + interstitial BT vs. SBRT
- PMID: 37381016
- PMCID: PMC10308761
- DOI: 10.1186/s13014-023-02295-4
Boost modalities in cervical cancer: dosimetric comparison between intracavitary BT vs. intracavitary + interstitial BT vs. SBRT
Abstract
Purpose / objective: This study compares the dosimetric plans of three distinct boost modalities in cervical cancer (CC): intracavitary (IC) with tandem/ovoids brachytherapy (BT), IC + interstitial (IS) BT, and Stereotactic-Body-Radiotherapy (SBRT). The aim is to determine the dosimetric impact in terms of target coverage and organ at risk (OAR) doses.
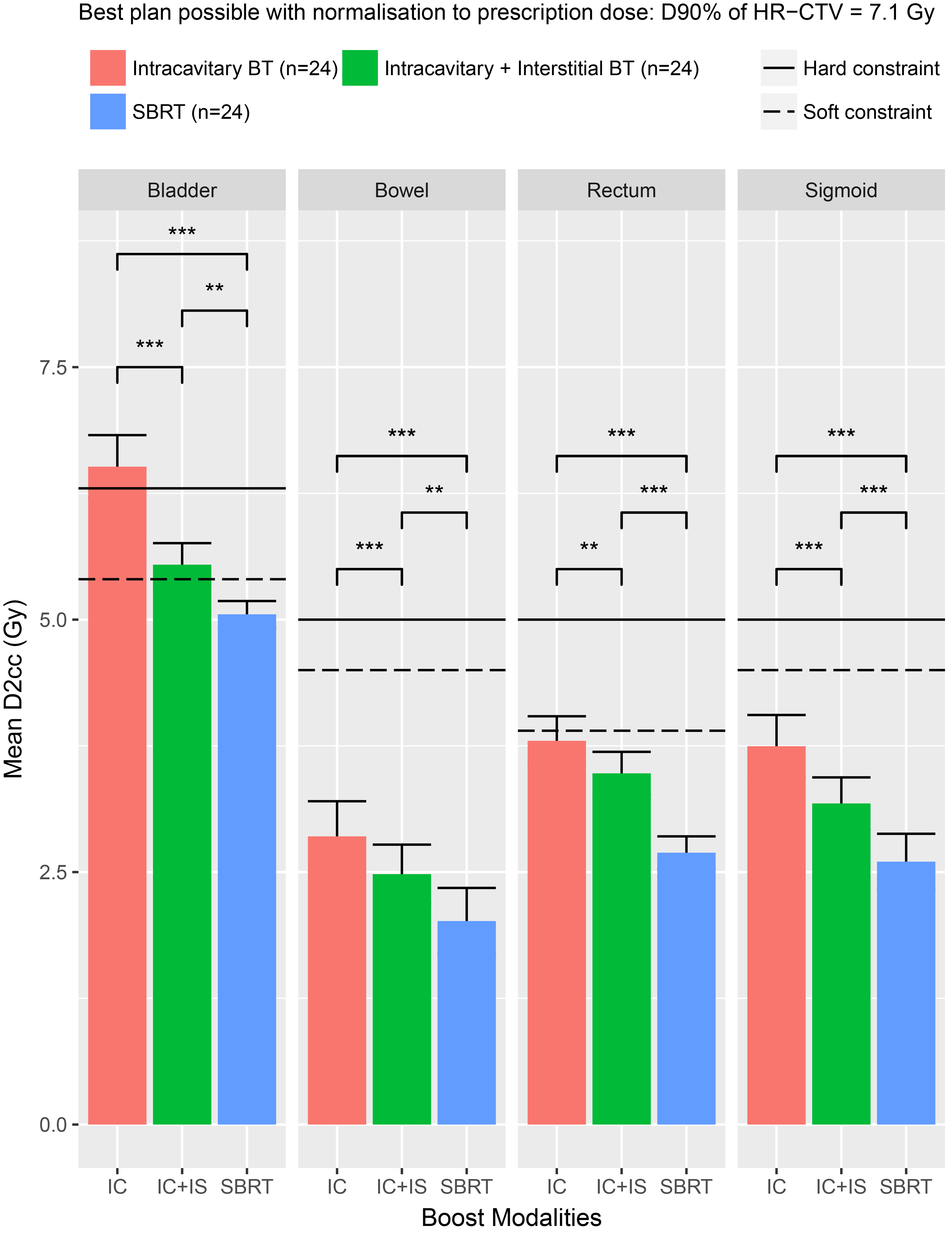
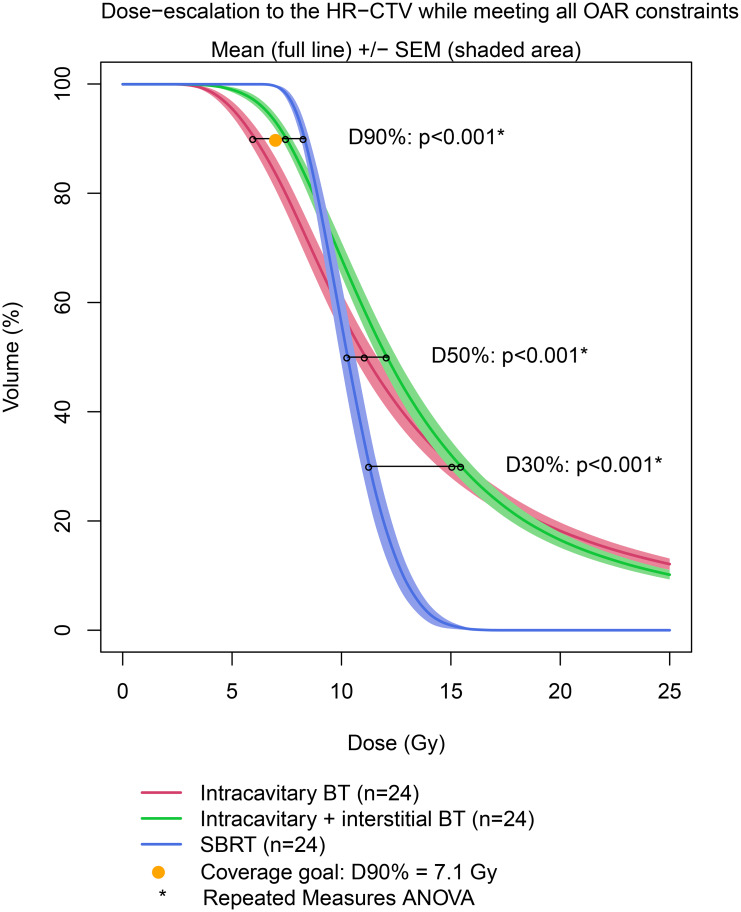
Materials and methods: 24 consecutive IC + IS BT boost treatment plans were retrospectively identified. For each plan included, two additional plans were created: IC-BT and SBRT. Importantly, no planning target volume (PTV) or planning (organ at) risk volume (PRV) margins were generated, therefore all structures were identical for any boost modality. Two different normalizations were performed: (1) Normalization to the target: prescription of 7.1 Gy to the D90% (defined as the minimum dose covering 90%) of the high-risk clinical target volume (HR-CTV); (2) Normalization to the OARs. HR-CTV coverage and OARs sparing were compared. The equivalent doses in 2 Gy fractions (EQD2) of EBRT and BT for CTV-HR and OARs were calculated using the linear-quadratic model with α/β of 10 (EQD210) and 3 (EQD23), respectively RESULTS: A total of 72 plans were investigated. In the first normalization, the mean EQD23-D2cc (defined as the minimal dose of the 2 cc) of OAR was significantly higher in the IC-BT plans, and the bladder D2cc hard constraint could not be reached. IC + IS BT leads to a 1 Gy mean absolute decrease of bladder EQD23-D2cc (relative dose: -19%), allowing to reach the hard constraint. SBRT (without PTV) delivers the lowest EQD23-D2cc to the OAR. In the second normalization, IC-BT provides a significantly lower dose to the EQD210-D90% (6.62 Gy) and cannot achieve the coverage goal. SBRT (without PTV) yields the highest dose to the D90% of HR-CTV and a significantly lower EQD210-D50% and D30%.
Conclusion: The key dosimetric benefit of BT over SBRT without PTV is a significantly higher D50% and D30% in the HR-CTV, which increases the local and conformal dose to the target. IC + IS BT vs. IC-BT provides significantly better target coverage and a lower dose to the OARs, making it the preferred boost modality in CC.
Keywords: Boost modalities; Brachytherapy; Cervical Cancer; Stereotactic body Radiotherapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cibula D, Pötter R, Planchamp F, Avall-Lundqvist E, Fischerova D, Haie Meder C, et al. The european Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the management of patients with cervical Cancer. Int J Gynecol Cancer Off J Int Gynecol Cancer Soc. 2018 May;28(4):641–55. - PubMed
-
- Gill BS, Lin JF, Krivak TC, Sukumvanich P, Laskey RA, Ross MS, et al. National Cancer Data Base analysis of radiation therapy consolidation modality for cervical cancer: the impact of new technological advancements. Int J Radiat Oncol Biol Phys. 2014 Dec;90(1):1083–90. - PubMed
-
- OʼDonnell B, Shiao JC, Pezzi TA, Waheed N, Sharma S, Bonnen MD, et al. Stereotactic body Radiation Therapy, intensity-modulated Radiation Therapy, and Brachytherapy Boost Modalities in Invasive Cervical Cancer: a study of the National Cancer Data Base. Int J Gynecol Cancer Off J Int Gynecol Cancer Soc. 2018 Mar;28(3):563–74. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
