

Mortality in Patients Hospitalized With Acute Myocardial Infarction Without Standard Modifiable Risk Factors: The ARIC Study Community Surveillance
- PMID: 37382152
- PMCID: PMC10356095
- DOI: 10.1161/JAHA.122.027851
Mortality in Patients Hospitalized With Acute Myocardial Infarction Without Standard Modifiable Risk Factors: The ARIC Study Community Surveillance
Abstract
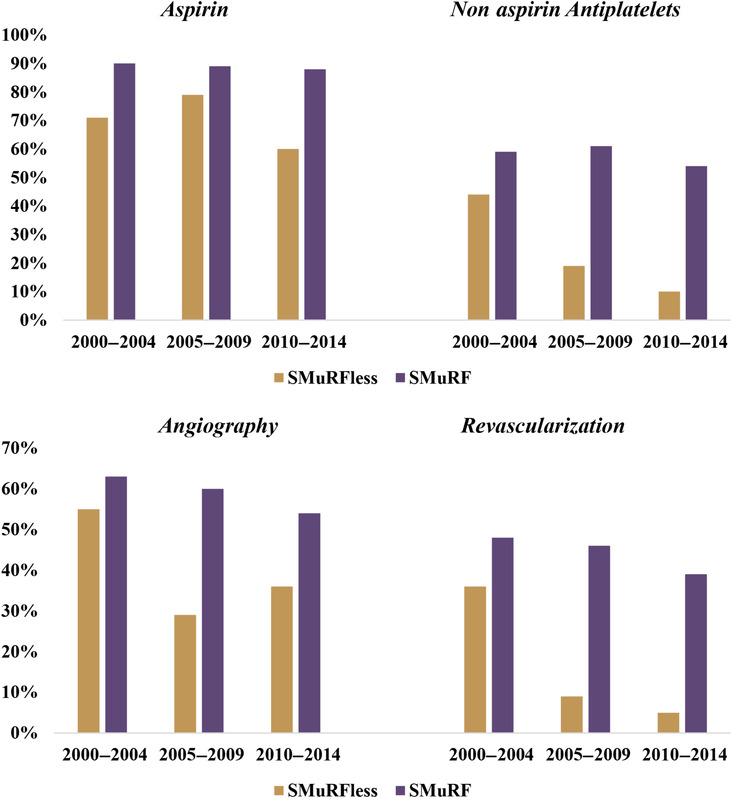
Background Prevention strategies targeting standard modifiable cardiovascular risk factors (SMuRFs; diabetes, hypertension, smoking, hypercholesterolemia) are critical to improving cardiovascular disease outcomes. However, acute myocardial infarction (AMI) among individuals who lack 1 or more SMuRFs is not uncommon. Moreover, the clinical characteristics and prognosis of SMuRFless individuals are not well characterized. Methods and Results We analyzed AMI hospitalizations from 2000 to 2014 captured by the ARIC (Atherosclerosis Risk in Community) study community surveillance. AMI was classified by physician review using a validated algorithm. Clinical data, medications, and procedures were abstracted from the medical record. Main study outcomes included short- and long-term mortality within 28 days and 1 year of AMI hospitalization. Between 2000 and 2014, a total of 742 (3.6%) of 20 569 patients with AMI were identified with no documented SMuRFs. Patients without SMuRFs were less likely to receive aspirin, nonaspirin antiplatelet therapy, or beta blockers and less often underwent angiography and revascularization. Compared with those with one or more SMuRFs, patients without SMuRFs had significantly higher 28-day (odds ratio, 3.23 [95% CI, 1.78-5.88]) and 1-year (hazard ratio, 2.09 [95% CI, 1.29-3.37]) adjusted mortality. When examined across 5-year intervals from 2000 to 2014, the incidence of 28-day mortality significantly increased for patients without SMuRFs (7% to 15% to 27%), whereas it declined for those with 1 or more SMuRFs (7% to 5% to 5%). Conclusions Individuals without SMuRFs presenting with AMI have an increased risk of all-cause mortality with an overall lower prescription rate for guideline-directed medical therapy. These findings highlight the need for evidence-based pharmacotherapy during hospitalization and the need to discover new markers and mechanisms for early risk identification in this population.
Keywords: acute coronary syndrome; acute myocardial infarction; cardiovascular disease; chest pain; standard modifiable risk factors.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
