

Eligibility for the 4 Pharmacological Pillars in Heart Failure With Reduced Ejection Fraction at Discharge
- PMID: 37382176
- PMCID: PMC10356099
- DOI: 10.1161/JAHA.122.029071
Eligibility for the 4 Pharmacological Pillars in Heart Failure With Reduced Ejection Fraction at Discharge
Abstract
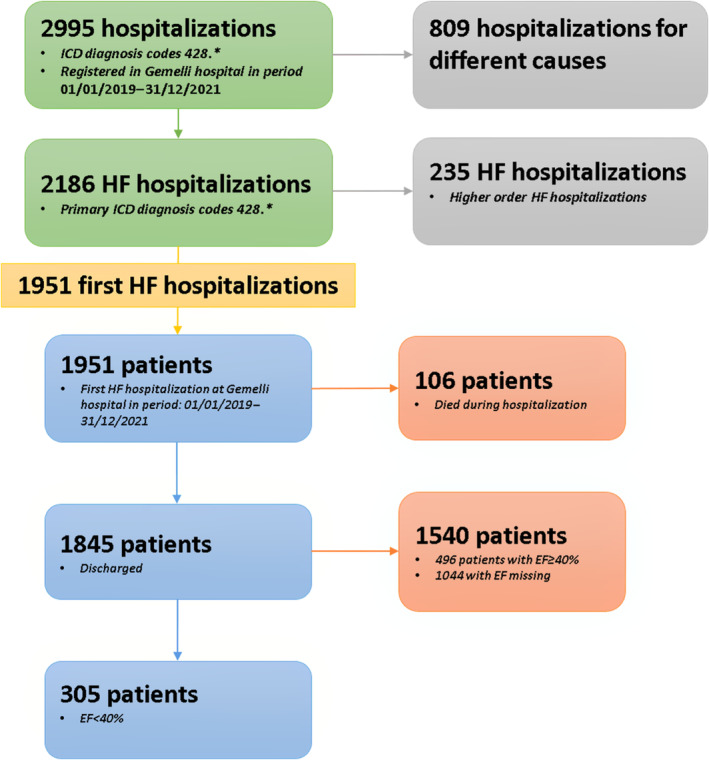
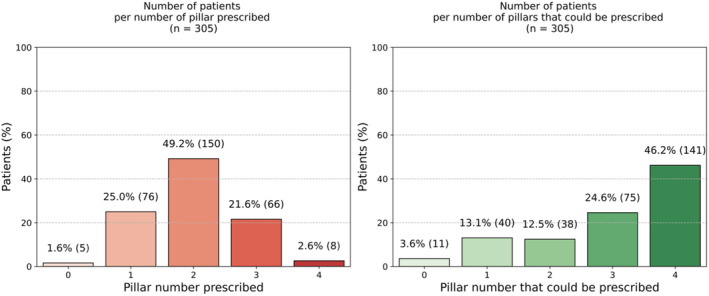
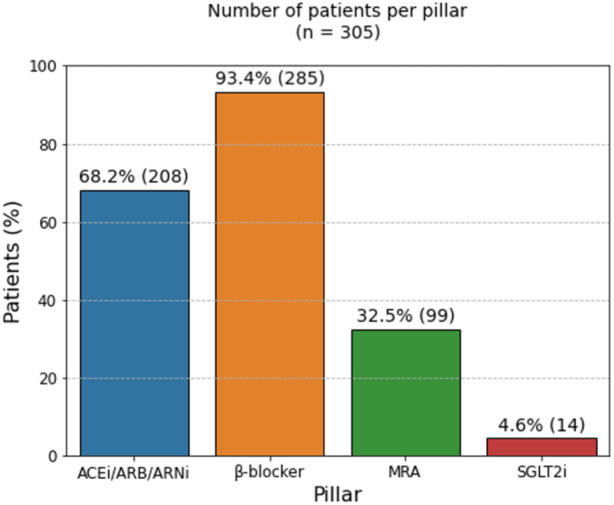
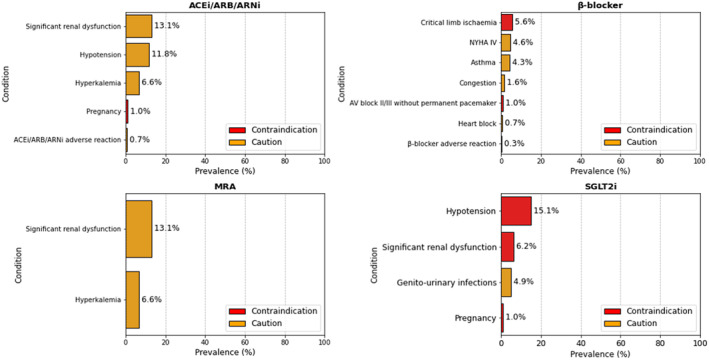
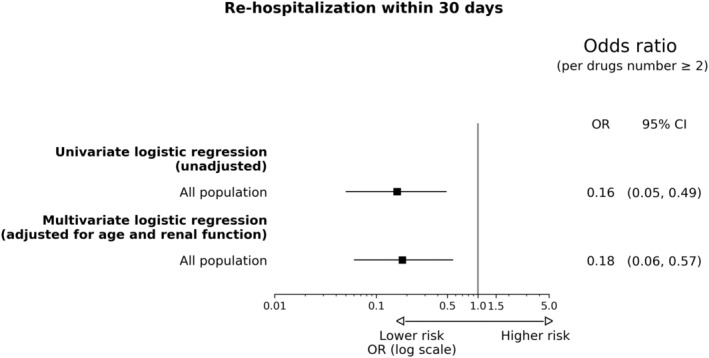
Background Guidelines recommend using multiple drugs in patients with heart failure (HF) with reduced ejection fraction, but there is a paucity of real-world data on the simultaneous initiation of the 4 pharmacological pillars at discharge after a decompensation event. Methods and Results A retrospective data mart, including patients diagnosed with HF, was implemented. Consecutively admitted patients with HF with reduced ejection fraction were selected through an automated approach and categorized according to the number/type of treatments prescribed at discharge. The prevalence of contraindications and cautions for HF with reduced ejection fraction treatments was systematically assessed. Logistic regression models were fitted to assess predictors of the number of treatments (≥2 versus <2 drugs) prescribed and the risk of rehospitalization. A population of 305 patients with a first episode of HF hospitalization and a diagnosis of HF with reduced ejection fraction (ejection fraction, <40%) was selected. At discharge, 49.2% received 2 current recommended drugs, β-blockers were prescribed in 93.4%, while a renin-angiotensin system inhibitor or an angiotensin receptor-neprilysin inhibitor was prescribed in 68.2%. A mineralocorticoid receptor antagonist was prescribed in 32.5%, although none of the patients showed contraindications to mineralocorticoid receptor antagonist prescription. A sodium-glucose cotransporter 2 inhibitor could be prescribed in 71.1% of patients. On the basis of current recommendations, 46.2% could receive the 4 foundational drugs at discharge. Renal dysfunction was associated with <2 foundational drugs prescribed. After adjusting for age and renal function, use of ≥2 drugs was associated with lower risk of rehospitalization during the 30 days after discharge. Conclusions A quadruple therapy could be directly implementable at discharge, potentially providing prognostic advantages. Renal dysfunction was the main prevalent condition limiting this approach.
Keywords: 4 pillars; cautions; comprehensive therapy; contraindications; heart failure with reduced ejection fraction.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
