

Prevalence, trends, and characteristics of trials investigating local therapy in contemporary phase 3 clinical cancer research
- PMID: 37382235
- PMCID: PMC11349322
- DOI: 10.1002/cncr.34929
Prevalence, trends, and characteristics of trials investigating local therapy in contemporary phase 3 clinical cancer research
Abstract
Background: Although most patients with cancer are treated with local therapy (LT), the proportion of late-phase clinical trials investigating local therapeutic interventions is unknown. The purpose of this study was to determine the proportion, characteristics, and trends of phase 3 cancer clinical trials assessing the therapeutic value of LT over time.
Methods: This was a cross-sectional analysis of interventional randomized controlled trials in oncology published from 2002 through 2020 and registered on ClinicalTrials.gov. Trends and characteristics of LT trials were compared to all other trials.
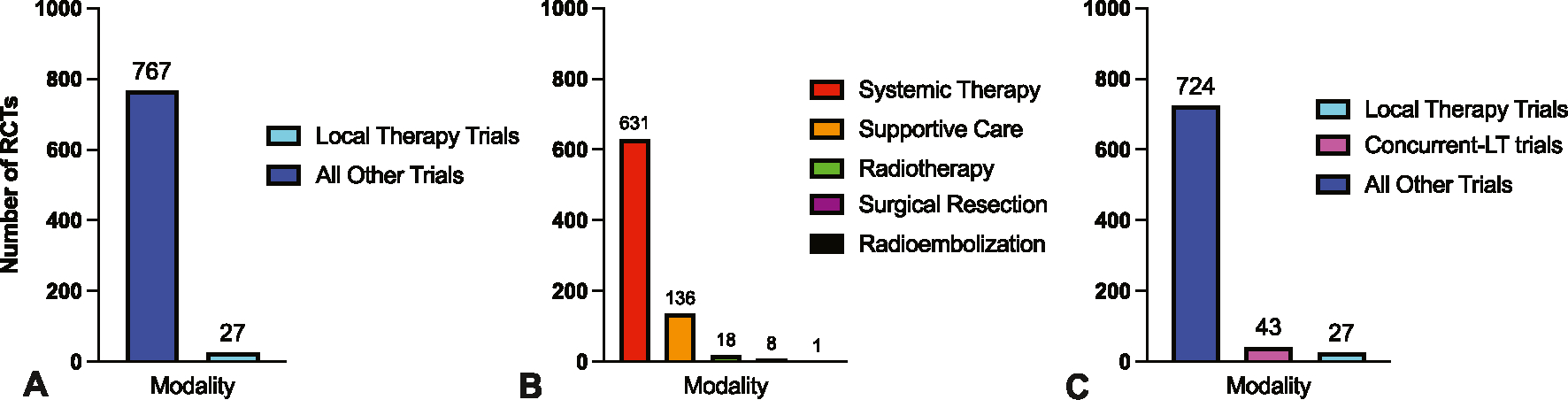
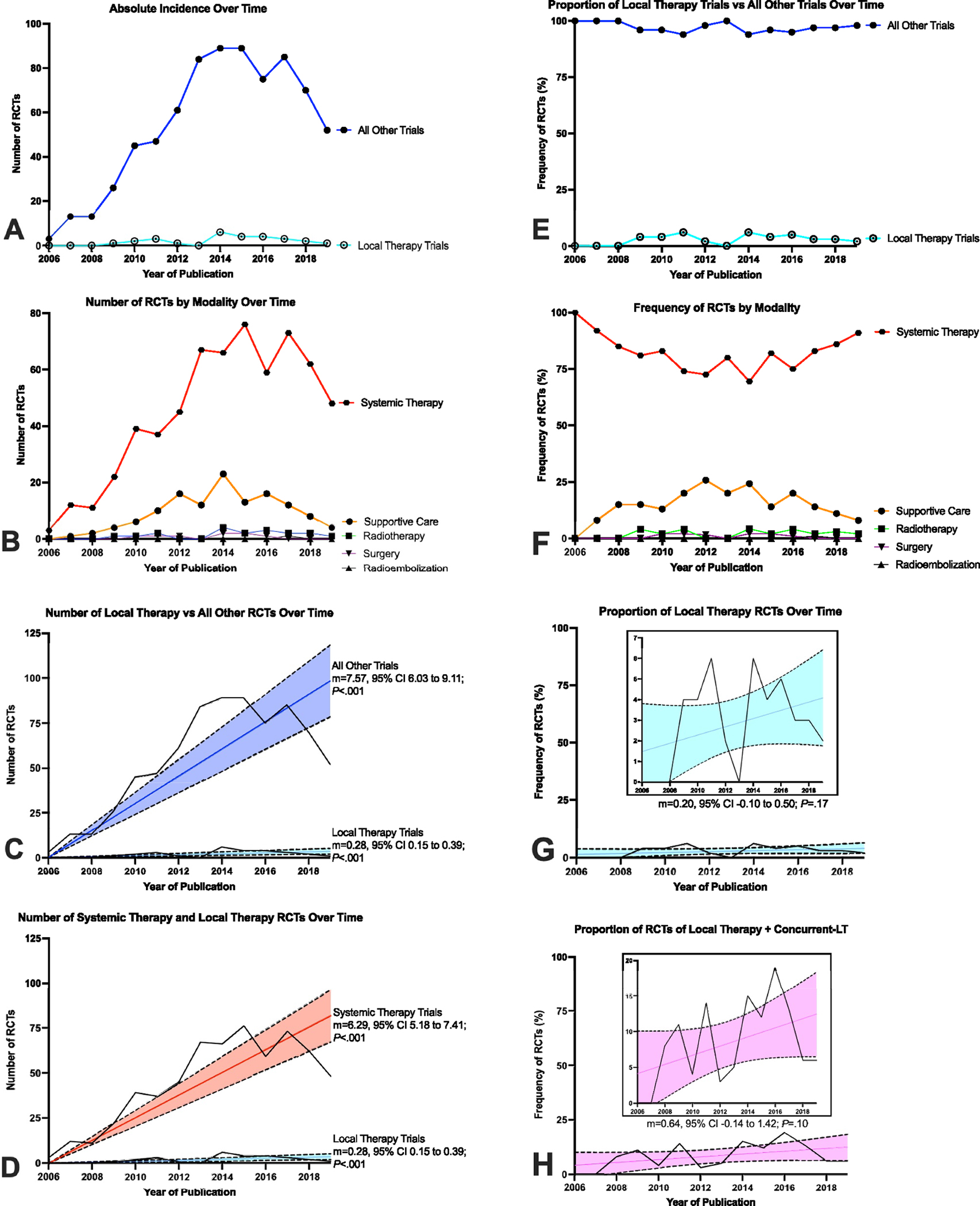
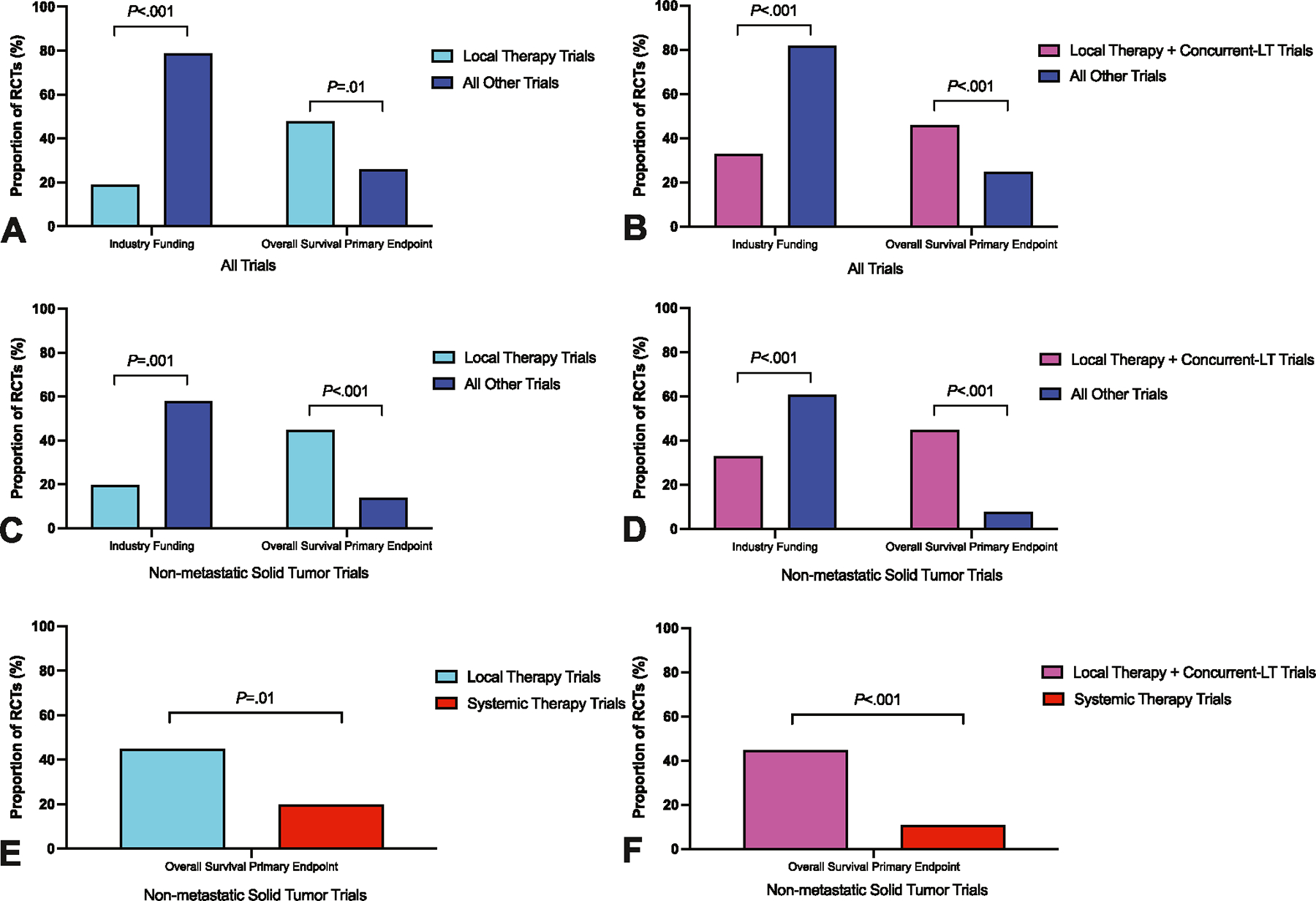
Results: Of 1877 trials screened, 794 trials enrolling 584,347 patients met inclusion criteria. A total of 27 trials (3%) included a primary randomization assessing LT compared with 767 trials (97%) investigating systemic therapy or supportive care. Annual increase in the number of LT trials (slope [m] = 0.28; 95% confidence interval [CI], 0.15-0.39; p < .001) was outpaced by the increase of trials testing systemic therapy or supportive care (m = 7.57; 95% CI, 6.03-9.11; p < .001). LT trials were more often sponsored by cooperative groups (22 of 27 [81%] vs. 211 of 767 [28%]; p < .001) and less often sponsored by industry (5 of 27 [19%] vs. 609 of 767 [79%]; p < .001). LT trials were more likely to use overall survival as primary end point compared to other trials (13 of 27 [48%] vs. 199 of 767 [26%]; p = .01).
Conclusions: In contemporary late-phase oncology research, LT trials are increasingly under-represented, under-funded, and evaluate more challenging end points compared to other modalities. These findings strongly argue for greater resource allocation and funding mechanisms for LT clinical trials.
Plain language summary: Most people who have cancer receive treatments directed at the site of their cancer, such as surgery or radiation. We do not know, however, how many trials test surgery or radiation compared to drug treatments (that go all over the body). We reviewed trials testing the most researched strategies (phase 3) completed between 2002 and 2020. Only 27 trials tested local treatments like surgery or radiation compared to 767 trials testing other treatments. Our study has important implications for funding research and understanding cancer research priorities.
Keywords: medical oncology; palliative care; phase 3 clinical trials; radiation oncology; randomized controlled trial; surgical oncology; trial design.
© 2023 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
Prajnan Das reports honoraria from the American Society of Clinical Oncology, the American Society for Radiation Oncology, the National Cancer Institute, Physicians Education Resource, Conveners, Imedex, and Bayer. C. David Fuller reports unrelated funding and salary support from National Institutes of Health National Institute of Biomedical Imaging and Bioengineering Research Education Programs for Residents and Clinical Fellows, a National Institute of Dental and Craniofacial Research Academic Industrial Partnership Grant, a NCI Parent Research Project Grant, an National Institutes of Health/National Cancer Institute Cancer Center Support Grant, and an National Science Foundation Division of Civil, Mechanical, and Manufacturing Innovation grant; direct industry grant support, honoraria, and travel funding from Elekta AB unrelated to this project; and direct infrastructure support from the multidisciplinary Radiation Oncology/Cancer Imaging Program of The MD Anderson Cancer Center and The MD Anderson Program in Image–Guided Cancer Therapy. Cullen Taniguchi reports consulting fees from Phebry and Xerient and holds a patent related to radioprotection of the upper gastrointestinal tract. The other authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
