

Burden and Treatment of Achondroplasia: A Systematic Literature Review
- PMID: 37382866
- PMCID: PMC10427595
- DOI: 10.1007/s12325-023-02549-3
Burden and Treatment of Achondroplasia: A Systematic Literature Review
Abstract
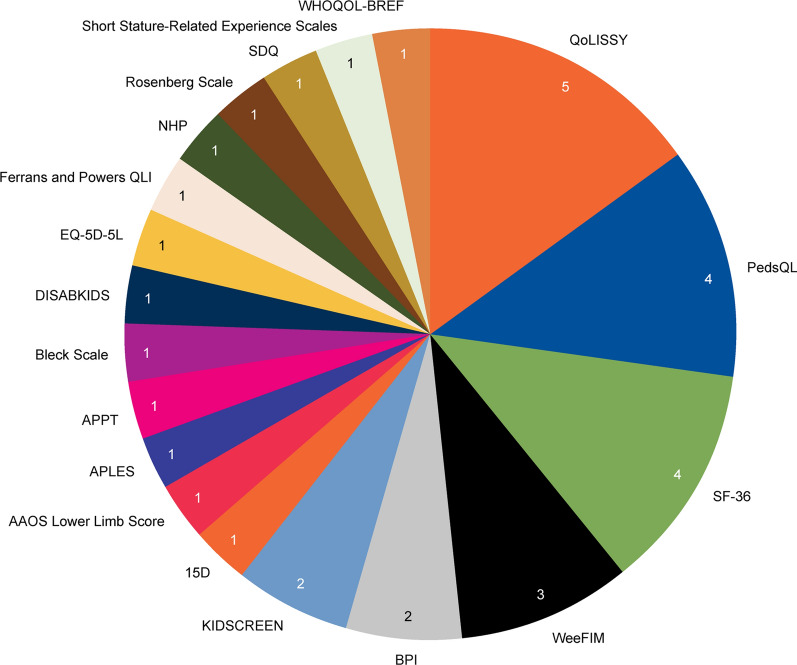
Background: Achondroplasia is the most common form of skeletal dysplasia. Recent advances in therapeutic options have highlighted the need for understanding the burden and treatment landscape of the condition. This systematic literature review (SLR) aimed to identify health-related quality of life (HRQoL)/utilities, healthcare resource use (HCRU), costs, efficacy, safety and economic evaluation data in achondroplasia and to identify gaps in the research.
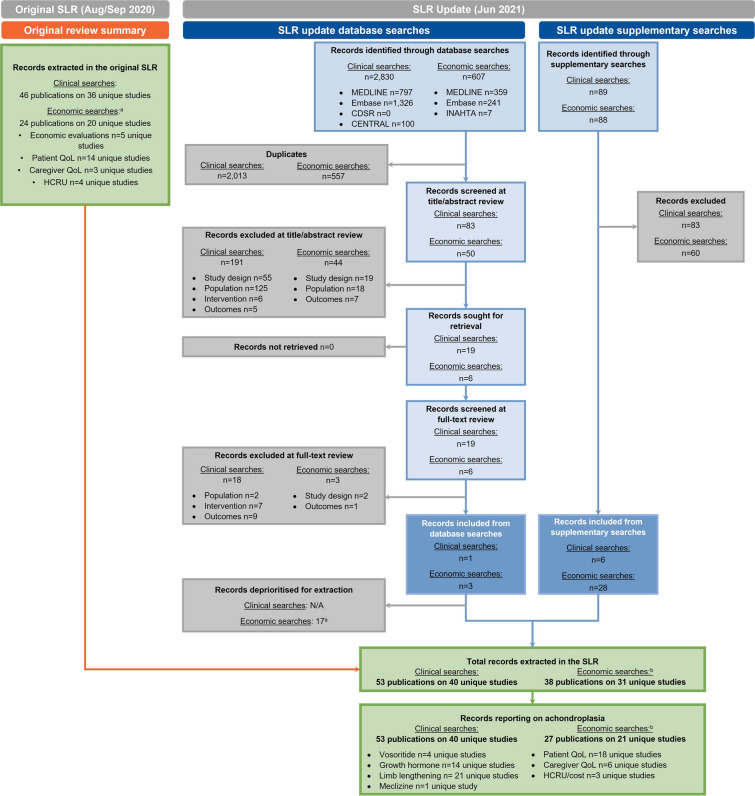
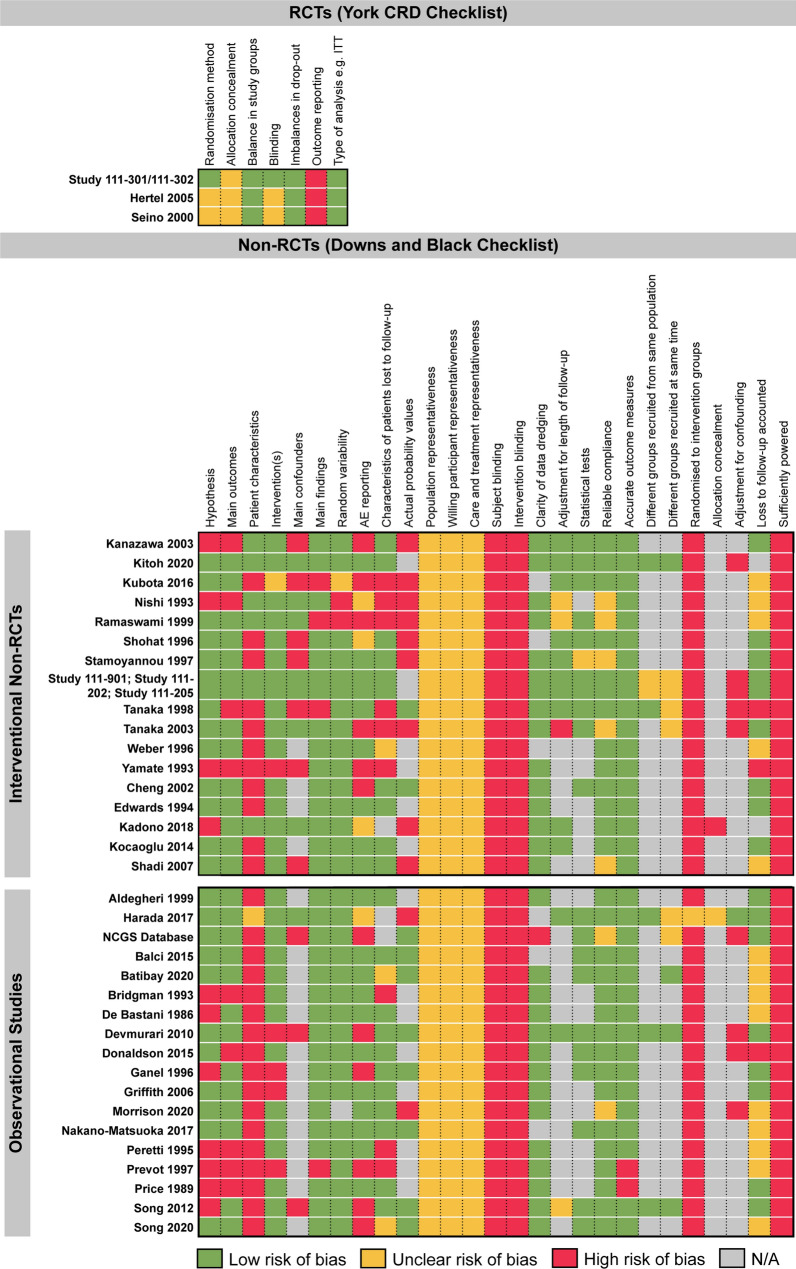
Methods: Searches of MEDLINE, Embase, the University of York Centre for Reviews and Dissemination (CRD), the Cochrane Library and grey literature were performed. Articles were screened against pre-specified eligibility criteria by two individuals and study quality was assessed using published checklists. Additional targeted searches were conducted to identify management guidelines.
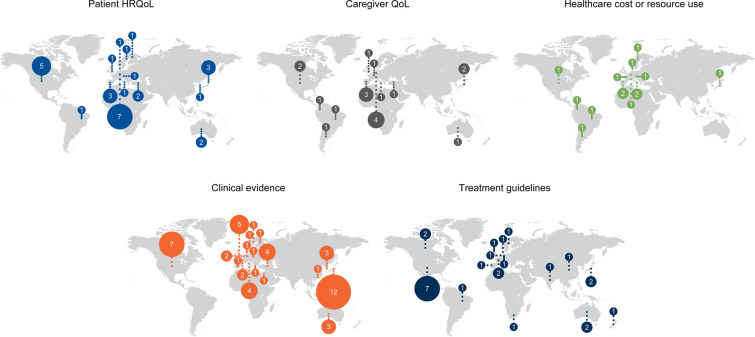
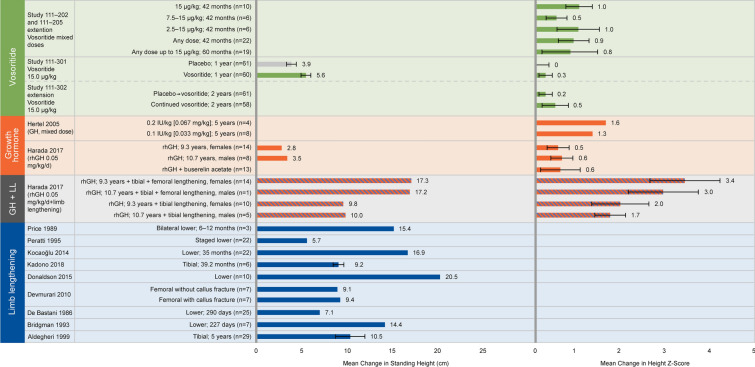
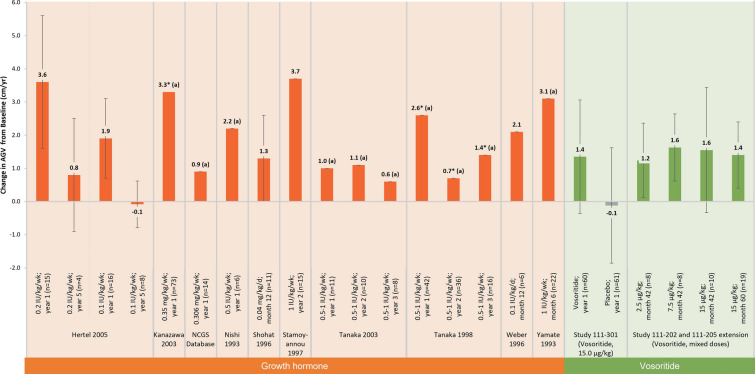
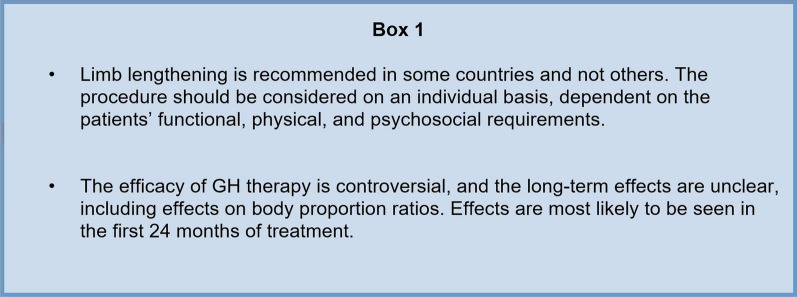
Results: Fifty-nine unique studies were included. Results demonstrated a substantial HRQoL and HCRU/cost-related burden of achondroplasia on affected individuals and their families throughout their lifetimes, particularly in emotional wellbeing and hospitalisation costs and resource use. Vosoritide, growth hormone (GH) and limb lengthening all conferred benefits for height or growth velocity; however, the long-term effects of GH therapy were unclear, data for vosoritide were from a limited number of studies, and limb lengthening was associated with complications. Included management guidelines varied widely in their scope, with the first global effort to standardise achondroplasia management represented by the International Achondroplasia Consensus Statement published at the end of 2021. Current evidence gaps include a lack of utility and cost-effectiveness data for achondroplasia and its treatments.
Conclusions: This SLR provides a comprehensive overview of the current burden and treatment landscape for achondroplasia, along with areas where evidence is lacking. This review should be updated as new evidence becomes available on emerging therapies.
Keywords: Achondroplasia; Disease overview; Dwarfism; Growth hormone; Limb lengthening; Short stature; Vosoritide.
© 2023. The Author(s).
Conflict of interest statement
Melita Irving has received honoraria for consultancy services from BioMarin, QED Therapeutics, Sanofi, Ascendis, Alexion, Kyowa Kirin, Innoskel, Novo Nordisk; Thomas Butt and Renée Shediac are employees and shareholders of BioMarin; Molly Murton, Emma Drane and Danielle Goff-Leggett are employees of Costello Medical. Jamie O’Hara has no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
