

Patient-Specific Pharmacokinetics and Dasatinib Nephrotoxicity
- PMID: 37382967
- PMCID: PMC10564352
- DOI: 10.2215/CJN.0000000000000219
Patient-Specific Pharmacokinetics and Dasatinib Nephrotoxicity
Abstract
Background: Dasatinib has been associated with nephrotoxicity. We sought to examine the incidence of proteinuria on dasatinib and determine potential risk factors that may increase dasatinib-associated glomerular injury.
Methods: We examined glomerular injury through urine albumin-creatinine ratio (UACR) in 82 patients with chronic myelogenous leukemia who were on tyrosine-kinase inhibitor therapy for at least 90 days. t tests were used to compare mean differences in UACR, while regression analysis was used to assess the effects of drug parameters on proteinuria development while on dasatinib. We assayed plasma dasatinib pharmacokinetics using tandem mass spectroscopy and further described a case study of a patient who experienced nephrotic-range proteinuria while on dasatinib.
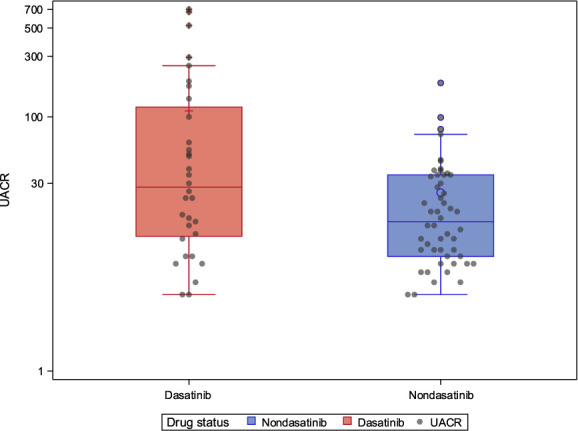
Results: Participants treated with dasatinib ( n =32) had significantly higher UACR levels (median 28.0 mg/g; interquartile range, 11.5-119.5) than participants treated with other tyrosine-kinase inhibitors ( n =50; median 15.0 mg/g; interquartile range, 8.0-35.0; P < 0.001). In total, 10% of dasatinib users exhibited severely increased albuminuria (UACR >300 mg/g) versus zero in other tyrosine-kinase inhibitors. Average steady-state concentrations of dasatinib were positively correlated with UACR ( ρ =0.54, P = 0.03) and duration of treatment ( P = 0.003). There were no associations with elevated BP or other confounding factors. In the case study, kidney biopsy revealed global glomerular damage with diffuse foot process effacement that recovered on termination of dasatinib treatment.
Conclusions: Exposure to dasatinib was associated with a significant chance of developing proteinuria compared with other similar tyrosine-kinase inhibitors. Dasatinib plasma concentration significantly correlated with higher risk of developing proteinuria while receiving dasatinib.
Podcast: This article contains a podcast at https://dts.podtrac.com/redirect.mp3/www.asn-online.org/media/podcast/CJASN/2023_09_08_CJN0000000000000219.mp3.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
M.H. Abramson reports employment with Icahn School of Medicine at Mount Sinai. B.O. Adegbite reports employment with Mount Sinai. E.U. Azeloglu reports employment with Icahn School of Medicine at Mount Sinai, consultancy for Ikena Oncology, ownership interest in Novartis, research funding from Aurinia Pharmaceuticals and Renalytix AI, patents or royalties from Mount Sinai Health System, and role on
Figures





Update of
-
Dasatinib nephrotoxicity correlates with patient-specific pharmacokinetics.medRxiv [Preprint]. 2023 Apr 17:2023.04.09.23288333. doi: 10.1101/2023.04.09.23288333. medRxiv. 2023. Update in: Clin J Am Soc Nephrol. 2023 Sep 1;18(9):1175-1185. doi: 10.2215/CJN.0000000000000219. PMID: 37131844 Free PMC article. Updated. Preprint.
References
-
- Cortes JE Jiang Q Wang J, et al. Dasatinib vs. imatinib in patients with chronic myeloid leukemia in chronic phase (CML-CP) who have not achieved an optimal response to 3 months of imatinib therapy: the DASCERN randomized study. Leukemia. 2020;34(8):2064–2073. doi: 10.1038/s41375-020-0805-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
