

Stereotactic laser ablation in neuro-oncology - A survey among European neurosurgeons
- PMID: 37383437
- PMCID: PMC10293215
- DOI: 10.1016/j.bas.2023.101749
Stereotactic laser ablation in neuro-oncology - A survey among European neurosurgeons
Abstract
Introduction: In the last decades, the application of stereotactic laser ablation (SLA) for the treatment of intracranial tumours has been growing, even though comparative trials are lacking. Our aim was to investigate the familiarity with SLA of neurosurgeons in Europe and their opinion regarding potential neuro-oncological indications. Furthermore, we investigated treatment preferences and variability for three exemplar neuro-oncological cases and willingness to refer for SLA.
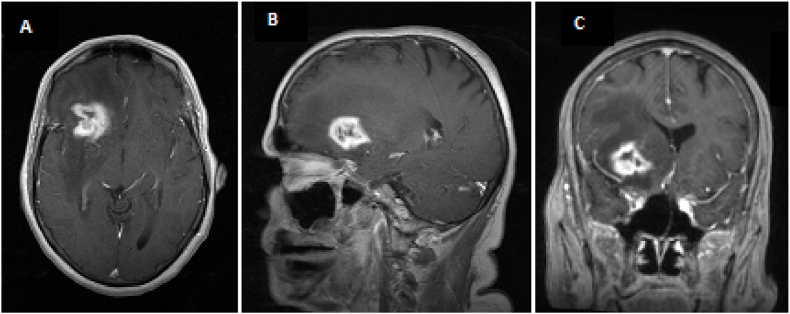
Material and methods: A 26-questions survey was mailed to members of the EANS neuro-oncology section. We presented three clinical cases of respectively deep-seated glioblastoma, recurrent metastasis and recurrent glioblastoma. Descriptive statistics was applied to report results.
Results: 110 respondents completed all questions. Recurrent glioblastoma and recurrent metastases were regarded as the most feasible indications for SLA (chosen by 69% and 58% of the respondents) followed by newly diagnosed high-grade gliomas (31%). Seventy percent of respondents would refer patients for SLA. The majority of respondents would consider SLA as a treatment option for all three presented cases: 79% for the deep-seated glioblastoma case, 65% for the recurrent metastasis case and 76% for the recurrent glioblastoma case. Among respondents who wouldn't consider SLA, preference for standard treatment and lack of clinical evidence were reported as the main reasons.
Conclusions: Most of respondents considered SLA as a treatment option for recurrent glioblastoma, recurrent metastases and newly diagnosed deep-seated glioblastoma. At the moment the current evidence to support such a treatment is very low. Comparative prospective trials are needed to support the use of SLA and determine proper indications.
Keywords: Glioblastoma; Neuro-oncology; Stereotactic laser ablation; Survey.
© 2023 The Authors. Published by Elsevier B.V. on behalf of EUROSPINE, the Spine Society of Europe, EANS, the European Association of Neurosurgical Societies.
Conflict of interest statement
The authors declare the following interests/personal relationships which may be considered as potential competing interests: We (IV, CO, ML) have previously been supported (in kind and financially) by Medtronic (r) for performing a laser ablation pilot trial (Grant ERP-2020-12244). Currently all authors are involved in a government funded RCT on laser ablations in glioblastoma, NCT05318612.
Figures




References
-
- Alattar A.A., Bartek J., Jr., Chiang V.L., Mohammadi A.M., Barnett G.H., Sloan A., Chen C.C. Stereotactic laser ablation as treatment of brain metastases recurring after stereotactic radiosurgery: a systematic literature review. World Neurosurg. 2019;128:134–142. - PubMed
-
- Ashraf O., Patel N.V., Hanft S., Danish S.F. Laser-Induced thermal therapy in neuro-oncology: a review. World Neurosurg. 2018;112:166–177. - PubMed
-
- Commission E. 2020. New EU Rules to Ensure Safety of Medical Devices.
-
- Franck P., Henderson P.W., Rothaus K.O. Basics of lasers history, physics, and clinical applications. Clin. Plast. Surg. 2016;43(3):505–+. - PubMed
LinkOut - more resources
Full Text Sources
