Update on Pathologic and Radiologic Diagnosis of Combined Hepatocellular-Cholangiocarcinoma
- PMID: 37384273
- PMCID: PMC10035725
- DOI: 10.17998/jlc.21.1.12
Update on Pathologic and Radiologic Diagnosis of Combined Hepatocellular-Cholangiocarcinoma
Abstract
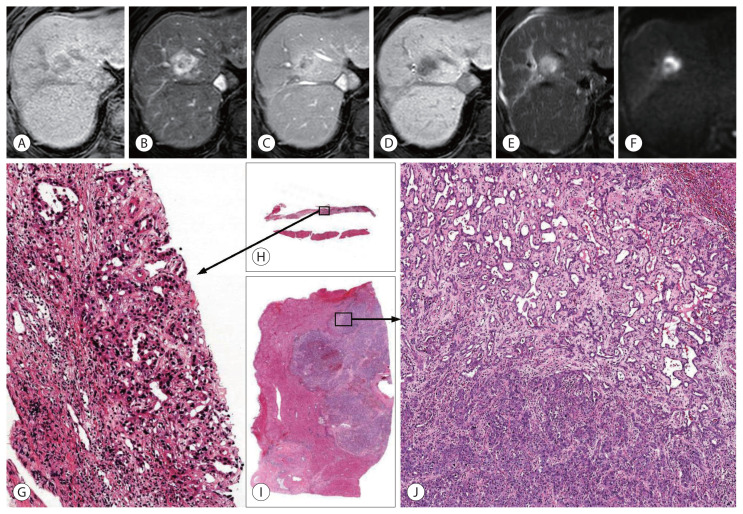
Combined hepatocellular-cholangiocarcinoma (cHCC-CCA) is a malignant primary liver carcinoma characterized by the unequivocal presence of both hepatocytic and cholangiocytic differentiation within the same tumor. Recent research has highlighted that cHCC-CCAs are more heterogeneous than previously expected. In the updated consensus terminology and WHO 2019 classification, "classical type" and "subtypes with stem-cell features" of the WHO 2010 classification are no longer recommended. Instead, it is recommended that the presence and percentages of various histopathologic components and stem-cell features be mentioned in the pathologic report. The new terminology and classification enable the exchange of clearer and more objective information about cHCC-CCAs, facilitating multi-center and multi-national research. However, there are limitations to the diagnosis of cHCC-CCA by imaging and biopsy. cHCC-CCAs showing typical imaging findings of HCC could be misdiagnosed as HCC and subjected to inappropriate treatment, if other clinical findings are not sufficiently considered. cHCC-CCAs showing at least one of the CCA-like imaging features or unusual clinical features should be subjected to biopsy. There may be a sampling error for the biopsy diagnosis of cHCC-CCA. An optimized diagnostic algorithm integrating clinical, radiological, and histopathologic information of biopsy is required to resolve these diagnostic pitfalls.
Keywords: Biopsy; Diagnosis; Liver neoplasm; Magnetic resonance imaging; Stem cell.
Copyright © 2021 by The Korean Liver Cancer Association.
Conflict of interest statement
Conflicts of Interest The authors declare no conflicts of interest relevant to this article.
Figures



Similar articles
-
Combined Hepatocellular-Cholangiocarcinoma: Changes in the 2019 World Health Organization Histological Classification System and Potential Impact on Imaging-Based Diagnosis.Korean J Radiol. 2020 Oct;21(10):1115-1125. doi: 10.3348/kjr.2020.0091. Epub 2020 Jul 27. Korean J Radiol. 2020. PMID: 32729276 Free PMC article. Review.
-
Combined Hepatocellular-Cholangiocarcinoma: An Update on Pathology and Diagnostic Approach.Biomedicines. 2022 Jul 29;10(8):1826. doi: 10.3390/biomedicines10081826. Biomedicines. 2022. PMID: 36009374 Free PMC article. Review.
-
Combined hepatocellular-cholangiocarcinoma: An update.J Hepatol. 2021 May;74(5):1212-1224. doi: 10.1016/j.jhep.2021.01.035. Epub 2021 Feb 3. J Hepatol. 2021. PMID: 33545267 Review.
-
Major and ancillary features according to LI-RADS in the assessment of combined hepatocellular-cholangiocarcinoma.Radiol Oncol. 2020 May 28;54(2):149-158. doi: 10.2478/raon-2020-0029. Radiol Oncol. 2020. PMID: 32463393 Free PMC article.
-
Combining imaging and tumour biopsy improves the diagnosis of combined hepatocellular-cholangiocarcinoma.Liver Int. 2019 Dec;39(12):2386-2396. doi: 10.1111/liv.14261. Epub 2019 Oct 20. Liver Int. 2019. PMID: 31544304
Cited by
-
MRI features of combined hepatocellular-cholangiocarcinoma.Abdom Radiol (NY). 2025 Jan;50(1):169-184. doi: 10.1007/s00261-024-04476-5. Epub 2024 Jul 20. Abdom Radiol (NY). 2025. PMID: 39031181 Review.
-
Imaging findings of intrahepatic cholangiocarcinoma for prognosis prediction and treatment decision-making: a narrative review.Ewha Med J. 2024 Oct;47(4):e66. doi: 10.12771/emj.2024.e66. Epub 2024 Oct 31. Ewha Med J. 2024. PMID: 40703995 Free PMC article. Review.
-
The Human TOR Signaling Regulator Is the Key Indicator of Liver Cancer Patients' Overall Survival: TIPRL/LC3/CD133/CD44 as Potential Biomarkers for Early Liver Cancers.Cancers (Basel). 2021 Jun 11;13(12):2925. doi: 10.3390/cancers13122925. Cancers (Basel). 2021. PMID: 34208132 Free PMC article.
-
Enhancing liver cirrhosis varices and CSPH risk prediction with spleen stiffness measurement using 100-Hz probe.Sci Rep. 2024 Jun 13;14(1):13674. doi: 10.1038/s41598-024-63848-5. Sci Rep. 2024. PMID: 38871788 Free PMC article.
-
Sarcomatoid change in combined hepatocellular carcinoma and cholangiocarcinoma as a poor prognostic factor.J Gastrointest Oncol. 2024 Aug 31;15(4):1796-1804. doi: 10.21037/jgo-24-313. Epub 2024 Aug 22. J Gastrointest Oncol. 2024. PMID: 39279943 Free PMC article.
References
-
- Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954;7:462–503. - PubMed
-
- Sempoux C, Kakar S, Kondo F, Schirmacher P. Combined hepatocellular-cholangiocarcinoma and undifferentiated primary liver carcinoma. World Health Organization, editor. WHO Classification of Tumours. (5th ed) 2019;1:260–262.
Publication types
LinkOut - more resources
Full Text Sources